

Essentials of Orthopedic Surgery, third edition / 11-The Hip and Femur
.pdf11
The Hip and Femur
BRIAN G. EVANS
The primary function of the lower extremities is locomotion. Any alteration of the function of the lower extremities will result in an alteration in the ability to walk and run. The hip is the most proximal joint in the lower extremity. Alteration in the hip as a result of disease will significantly effect the biomechanics of gait and place abnormal stress on the joints above and below the hip.
This chapter briefly reviews the anatomy of the hip and its relationship to normal and pathologic gait. The important history and physical examination findings of hip pathology are discussed. Diseases affecting the hip are reviewed and their treatment outlined. Surgical management of endstage disease of the hip commonly are treated by one of several options, and these are reviewed. The indications and outcome for each treatment option are also reviewed. In addition, trauma to the pelvis, acetabulum, and proximal femur are summarized and treatment alternatives outlined.
Anatomy
Development
The hip joint is a ball-and-socket joint with the round femoral head articulating within the round acetabular socket. The acetabulum is formed from the confluence of three bones: the ischium, the ilium, and the pubis. In skeletally immature patients these three bones are joined in the medial acetabulum by the triradiate cartilage, which is a growth plate for the acetabulum. There is also appositional growth from the edges of the acetabulum and pelvis, resulting in increased depth of the acetabulum and size of the pelvis. Normal development of the acetabulum requires the femoral head to articulate with the acetabular cartilage. If the femoral head is chronically dislocated or subluxed within the acetabular fossa, the acetabular socket does not develop fully, resulting in developmental dysplasia of the hip (DDH). The severity of this condition is determined by the degree of subluxation of the femoral head. If DDH is identified at birth or soon
415

416 B.G. Evans
thereafter, the hip can be reduced either with casting or surgery. This treatment can allow the hip to grow and develop almost normally. If the hip is left subluxed or dislocated, the acetabulum will be shallow and predispose the patient to develop osteoarthritis as an adult. This condition is reviewed in greater detail in the chapter on pediatric orthopedic conditions.
Osteology and Musculature
The innominate bone consists of the ilium, ischium, and pubis, which are joined in the area of the acetabulum (Fig. 11-1). The ilium is a large flat bone providing broad surfaces for muscular attachment. The ischium extends posteriorly and forms the posterior aspect of the acetabulum. The ischium joins the ilium superiorly and the pubis inferiorly through the inferior pubic ramus. The ischium also serves as the origin of the hamstring and short external rotator muscles of the hip. The pubis consists of the superior pubic ramus, the inferior pubic ramus, and the pubic symphysis. The superior pubic ramus joins the pubic symphysis with the ilium, and the inferior pubic ramus connects the pubic symphysis with the ischium. The pubis serves as the site of insertion of the musculature of the abdominal wall as well as the site of origin for the adductor muscles of the thigh.
|
Outer lip |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Iliac |
of iliac crest |
|
|
|
|
|
|
|
|
|
|
|
|
|
Obliquus |
||||
|
|
|
|
|
|
|
|
|
|
|
Obliquus |
|
|||||||
crest |
|
Anterior |
|
|
|
|
|
|
abdominis |
|
abdominis |
||||||||
|
|
gluteal line |
|
|
|
|
|
|
externus |
|
internus |
||||||||
|
|
|
|
|
|
|
|
|
Latissimus |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
dorsi |
|
|
|
|
|
|
|
|
|
Tensor fasciae |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Gluteus |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
latae |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
medius |
|
|
|
|
|
|
Anterior superior |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
iliac spine |
|
|
|
|
|
Gluteus |
|
Ilium |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sartorius |
|
|
|
|
|
|
maximus |
|
|
|
|
|
|
|
|
|
|
|
|
Gluteus |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Posterior |
||
|
|
|
|
|
|
|
|
|
|
|
|
minimus |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
superior |
||
|
|
|
|
|
|
|
|
Rectus femoris |
|
|
|
||||||||
Inferior |
|
|
|
|
|
|
|
|
|
|
illiac spine |
||||||||
|
|
|
Posterior |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
gluteal |
|
|
|
gluteal line |
|
|
|
|
|
|
|
|
|
|
|
|
Piriformis |
||
|
|
|
Anterior inferior |
|
|
||||||||||||||
line |
|
|
|
Acetabulum |
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
iliac spine |
|
|
Posterior |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Pubic |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
inferior |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Acetabular |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
Junction of ilium, |
|
illiac spine |
||||||||||
tubercle |
|
|
|
|
|
|
|
|
|||||||||||
|
|
notch |
|
|
|
|
|
pubis, and ischium |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
Gemellus superior |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ischium |
|
|
|
|
|
|
Pectineus |
|
|||||||
|
|
|
|
|
|
Rectus abdominis, |
|
|
|
Semimembranosus |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
lateral head |
|
|
|
|
|
Biceps |
|
|
|
|
|
|
|
|
|
|
|
Pyramidalis |
|
||||||||
|
|
|
|
|
Ischial |
|
|
|
|
|
|||||||||
Pubis |
|
|
|
|
|
|
|
|
|
|
Adductor |
|
|
|
|
|
femoris and |
||
|
|
|
|
tuberosity |
|
|
|
|
|
semitendinosus |
|||||||||
|
|
|
|
|
|
|
longus |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Quadratus femoris |
||
Obturator foramen |
|
|
|
|
|
|
|
Adductor brevis |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
Gracilis |
|
Obturator externus |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Junction of |
Adductor magnus |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ANTERIOR |
POSTERIOR |
|
|
|
|
|
|
ANTERIOR |
pubis and ischium |
POSTERIOR |
|||||||||
A |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
||||||
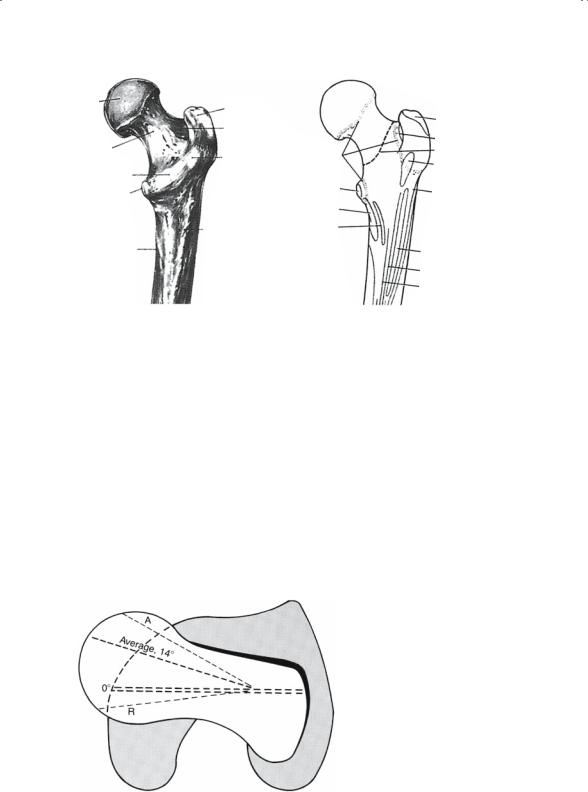
FIGURE 11-1. (A) Lateral aspect of left hip bone. (B) Attachments and epiphyseal lines are shown. (From Willams PL, Warwick R: Gray’s Anatomy, ed 36. Churchill Livingstone, 1980, pp 378–379. Reprinted by permission. From Steinberg M (ed). The Hip and Its Disorders. Philadelphia, WB Saunders Company, 1991, P 32. Reprinted by permission.)

|
11. The Hip and Femur |
417 |
||
Fovea on |
Piriformis |
|
|
|
head |
|
|
||
Head |
|
|
|
|
Greater |
|
|
|
|
trochanter |
Gluteus |
|
|
|
Neck |
|
|
||
minimus |
Epiphyseal |
|||
|
||||
Intertrochanteric |
|
|||
|
lines |
|
||
line |
|
|
||
|
Psoas |
|
||
|
Vastus |
|
||
Lesser trochanter |
major |
|
||
|
lateralis |
Vastus |
|
|
|
Capsular |
medialis |
||
|
|
|
||
attachment
FIGURE 11-2. (A) Anterior aspect of proximal right femur. (B) Attachments and epiphyseal lines. (From Willams PL, Warwick R. Gray’s Anatomy, ed 36. Churchill Livingstone, 1980, pp 392–393. Reprinted by permission. From Steinberg M (ed) The Hip and Its Disorders. Philadelphia, WB Saunders Company, 1991, p 28. Reprinted by permission.)
The acetabulum is formed at the junction of the ilium, ischium, and pubis. The ilium forms the superior dome of the acetabulum. The ischium forms the posterior acetabulum and the pubis the anterior acetabulum. The lateral opening of the acetabulum forms a horseshoe with the open end directed inferiorly. The medial base of the acetabulum contains a depression called the acetabular fovea, which is filled with a fatty tissue called the pulvinar and the ligamentum teres. The ligamentum teres is a ligament that extends from the acetabular fovea and the fovea of the femoral head.
The artery of the ligamentum teres is a branch of the obturator artery and supplies approximately 10% to 20% of the bone of the femoral head.
The fovea of the femur is a depression on the femoral head that serves as the site of attachment of the ligamentum teres. Attached to the rim of the horseshoe is a fibrocartilaginous labrum, which is similar to the meniscus in the knee. This structure serves to improve stability and to cushion the femoral neck when the femur is rotated and impinges upon the acetabular rim at the extremes of motion. The hip joint capsule is a dense fibrous structure extending from the base of the intertrochanteric region of the femur to the acetabular rim. Thickenings within the capsule are the iliofemoral and pubofemoral ligaments anteriorly and the ischiofemoral ligament posteriorly. These ligaments as well as the ligamentum teres and the labrum augment the stability of the hip joint.
The femoral head is essentially spherical in geometry (Figs. 11-2, 11-3). The spherical portion of the femoral head is covered by articular cartilage. The sphere is altered in two areas, laterally where the femoral neck begins
418 |
B.G. Evans |
|
|
|
Head |
|
Greater |
|
|
|
|
trochanter |
|
Gluteus medius |
|
|
Trochanteric |
|
|
|
|
|
|
|
|
|
fossa |
|
Obturator externus |
Neck |
|
Quadrate |
Epiphyseal |
Capsular attachment |
Intertrochanteric |
tubercle |
lines |
Quadratus femoris |
|
|
|
|
||
|
crest |
|
Psoas |
|
Lesser |
|
major |
Vastus lateralis |
|
trochanter |
|
Iliacus |
|
|
|
|
|
|
|
|
|
Gluteal |
Pectineus |
|
|
|
tuberosity |
|
|
Spiral line |
Gluteus maximus |
|
|
|
Adductor magnus |
|
Adductor brevis |
FIGURE 11-3. (A) Posterior aspect of proximal right femur. (B) Attachments and epiphyseal lines. (From Willams PL, Warwick R: Gray’s Anatomy, ed 36. Churchill Livingstone, 1980, p 394. Reprinted by permission. From Steinberg M (ed) The Hip and Its Disorders. Philadelphia, WB Saunders Company, 1991, p 28. Reprinted by permission.)
and medially at the fovea of the femoral head. The femoral neck joins the femur at an angle of approximately 125 degrees. The neck is also rotated anteriorly 12 to 14 degrees relative to the axis represented by the posterior femoral condyles (Fig. 11-4). The femoral neck flares laterally to join the proximal femur in between the greater and lesser trochanters. The greater trochanter, a large osseous prominence at the proximal lateral aspect of the femur, serves as the site of attachment of the abductor musculature.
Between the greater and lesser trochanters is an osseous ridge that serves
FIGURE 11-4. Average rotary, or torsion, angle of the femur. It may be anteverted (A) or retroverted (R). (From Steinberg M (ed) The Hip and Its Disorders. Philadelphia, WB Saunders Company, 1991, p 29. Reprinted by permission.)

11. The Hip and Femur |
419 |
as the site of attachment of the short external rotators. The lesser trochanter is the site of attachment of the iliopsosas tendon. This tendon leaves the pelvis over the anterior column and superior pubic ramus and then travels over the anterior femoral neck to insert on the lesser trochanter, which lies on the posterior inferior aspect of the intertrochanteric ridge. Within the proximal femur and femoral neck is a large and dense trabecula known as the calcar. The calcar provides increased strength to the proximal femur. Frequently the proximal posteromedial femur from the base of the femoral neck including the lesser trochanter is also referred to as the calcar. If the calcar region of the proximal femur is a separate fragment of a proximal femur fracture, this usually implies that the fracture is very unstable.
The muscles of the hip form several distinct groups. The anterior muscles are the hip flexors, which consist of the iliopsoas and rectus femoris and sartorius muscles. The femoral nerve innervates the rectus and sartorius muscles. Motor branches from spinal roots L2, L3, and L4 innervate the iliopsoas. The lateral group consists of the abductors, the gluteus medius, minimus, and tensor fascia lata. These muscles are essential for normal gait. They stabilize the pelvis in the single limb stance phase of normal gait. The anterior one-third of the gluteus medius muscle is also the principal internal rotator of the hip. The superior gluteal nerve innervates the gluteus medius, minimus, and tensor fascia lata. Surgical dissection that extends greater than 5 cm proximal to the greater trochanter can disrupt the nerve and result in a limp.
The posterior muscles are in two layers. The superficial layer consists of the gluteus maximus, the primary extensor of the hip, which is innervated by the inferior gluteal nerve. The deep layer consists of the short external rotators of the hip, the piriformis, superior gemellus, obturator internus, inferior gemellus, obturator externus, and the quadratus femoris and gluteus minimus and medius. These muscles externally rotate the femur and provide abduction. Small branches from the sacral plexus innervate the short external rotators. The medial muscle group consists of the pectineus, the adductor brevis, longus, and magnus, and the gracillis. The adductors and gracillis are supplied by the obturator nerve, with the posterior portion of the adductor magnus also receiving innervation from the tibial division of the sciatic nerve. The femoral nerve innervates the pectineus.
The sciatic nerve crosses the hip joint posteriorly. It exits the pelvis through the superior sciatic notch, under the piriformis muscle, and lies superficial to the short external rotators. The nerve has two distinct divisions within the single nerve sheath, the tibial and peroneal divisions. The peroneal division is more susceptible to injury, compared to the tibial division, at all levels along the course of the sciatic nerve. The increased susceptibility is the result of the more-lateral location and a more-tenuous blood supply of the peroneal division within the sciatic nerve sheath.

420 B.G. Evans
Therefore, a partial injury to the sciatic nerve commonly results in a foot drop, clinically similar to the deficits seen in an isolated injury to the common peroneal nerve injury at the level of the fibular neck. One anatomic point with important clinical relevance is that the peroneal division of the sciatic nerve has only one motor branch in the posterior thigh supplying the short head of the biceps. Determining if the short head of the biceps is normally innervated can assist in determining the level of peroneal nerve injury clinically (i.e., the hip or knee).
Vascular Anatomy of the Proximal Femur and
Femoral Head
The medial and lateral femoral circumflex vessels in conjunction with the artery of the ligamentum teres provide the vascular supply to proximal femur and femoral head (Fig. 11-5). The medial femoral circumflex artery extends posteriorly and ascends proximally deep to the quadratus femoris muscle. At the level of the hip it joins an arterial ring at the base of the femoral neck. The lateral femoral circumflex artery extends anteriorly and gives off an ascending branch, which also joins the arterial ring at the base
Lateral (superior) ascending cervical artery
|
Posterior ascending |
|
Muscular branches |
cervica artery |
|
Medial (interior) ascending |
||
to obturator externus |
||
cervical artery |
||
|
||
|
Medial femoral |
|
|
circumflex artery |
|
|
Lateral femoral |
|
|
circumflex artery |
FIGURE 11-5. Arterial supply to the head and neck of the posterior aspect of the left proximal femur. Note the extracapsular arterial ring on the surface of the capsule, the ascending cervical arteries on the neck of the femur, and the intraarticular sub-synovial arterial ring at the articular cartilage margin. (From Steinberg M (ed) The Hip and Its Disorders. Philadelphia, WB Saunders Company, 1991, p 19.)

11. The Hip and Femur |
421 |
of the femoral neck. This vascular ring gives rise to a group of vessels that run in the retinacular tissue inside the capsule to enter the femoral head at the base of the articular surface. These vessels provide 80% to 90% of the blood supply to the femoral head. The artery of the ligamentum teres, a branch of the obturator artery, travels within the ligamentum teres and supplies only 10% to 20% of the blood supply to the femoral head.
Biomechanics
The joint reaction force is the sum of all the forces that cross a joint, including components from gravity, body weight, and muscle forces acting upon the joint. In two-legged stance with both feet on the ground and static conditions, a joint reaction force of approximately 1.3 to 1.5 times body weight will cross each hip joint. However, in single-limb stance this force increases to 2.5 to 3 times body weight across the hip joint. The primary contribution to the increase is the force generated by the abductor muscles to maintain balance and to keep the pelvis level. If the system is in motion, such as with walking, the joint reaction forces can be as high as 4 times body weight.
Several studies have measured the actual joint reaction forces during rehabilitation using an implanted instrumented prosthesis. The greatest joint reaction force was noted when the patients arose from a low chair or during stair climbing. However, even nonweight-bearing activities such as getting onto a bedpan were found to have a joint reaction force of 1.5 to 1.8 times body weight. The lowest joint reaction forces with ambulation were recorded when patients used touch-down weight-bearing. Touchdown weight-bearing allows the patient to rest the foot on the ground to balance the weight of the leg but not to step down or weight-bear on the involved lower extremity.
Gait
The principal function of the lower extremities is ambulation. In gait analysis, a gait cycle examines one leg, beginning with heel strike and continuing until the next heel strike of the same leg. Gait can be divided into two principal phases, stance and swing. The stance phase is defined as that portion of the gait cycle when the foot is in contact with the ground. The swing phase is therefore the portion of each step when the foot is not in contact with the ground. The stance phase makes up 60% of each step with the remainder being made up by the swing phase. Therefore, during 20% of the gait cycle both feet are in contact with the ground. Normal gait requires a stable pelvis, which is provided by the hip abductor muscles. Normal gait also requires 40 degrees of hip flexion and 10 degrees of internal rotation and external rotation.

422 B.G. Evans
Patient Evaluation
History
The evaluation of a patient with hip pain requires careful attention to the history, physical examination, and radiographic studies. The character, nature, and duration of the patient’s pain should be documented. Acute or recent-onset pain is more commonly associated with trauma or infection.
Chronic and gradually progressive pain is associated with arthritic conditions. Intraarticular pain is usually described as a deep aching pain. Pain from the hip joint is commonly noted anteriorly in the groin or in the region of the greater trochanter. Hip pain can radiate down the inner and anterior thigh to the knee with little or no pain in the area of the hip. Only rarely does hip pain radiate distal to the knee. In adolescent patients, it is not uncommon for hip pathology to present as knee pain. Therefore, a thorough physical and radiographic evaluation of the hips is necessary to identify the pathology in these patients. Posterior pain and buttock pain is more commonly associated with lumbar spine pathology. Spine pain also more commonly radiates down the posterior thigh and below the knee. The insidious onset of a deep boring pain and pain that awakens the patient at night suggest either infection or neoplastic disease.
Hip pain is commonly aggravated by activity and relieved by rest. Patients will report difficulty donning and doffing their shoes and socks and difficulty with toenail care on the involved extremity. As the pain progresses, patients begin to have pain with prolonged sitting and at night as they try to sleep. Patients with hip arthritis will report that, if they sit for a prolonged period of time, when they get up to walk the hip feels out of place or painful for the first few steps. This feeling usually resolves quickly after a few minutes of walking.
The use of a cane, walking stick, or crutch should be documented. The patient may also have begun to take over-the-counter antiinflammatory medication or pain relievers. The medication and the amount the patient is taking as well as the level of relief this provided needs to be recorded. The patient’s walking tolerance can be measured in terms of blocks the patient can walk or in terms of how many minutes the patient can be ambulatory doing activities such as grocery shopping or walking in a mall. Documentation of these data will give a detailed picture of the degree of pain and the patient’s functional limitations.
Patients should also be questioned about past problems with the hip such as hip dislocation at birth, delays in ambulation as an infant, and any bracing as a child. Previous surgery or trauma to the hips should be explored in detail. The past medical history and any medications the patient is taking should be noted. This information can have implications for the patient’s hip problems and may have an impact upon what treatment may be instituted.

11. The Hip and Femur |
423 |
Physical Examination
The most important aspect of the physical examination in patients with hip disease is to evaluate their gait pattern as this reveals important information about the patient’s ambulatory status and pain. Patients with significant hip pain manifest a coxalgic gait. This gait pattern is represented by a reduced stance phase on the painful leg, and the shoulders will lurch laterally over the affected hip. Patients with mild pain or weakness in the abductor muscles may have a stance phase equal to the opposite leg but the shoulders will continue to lurch over the affected leg. This lurch results in moving the center of gravity closer to the center of rotation of the hip, which in turn reduces the force necessary to stabilize the pelvis in stance phase. This gait is referred to as a Trendelenburg gait (equal stance phase and the shoulders lurching over the affected hip).
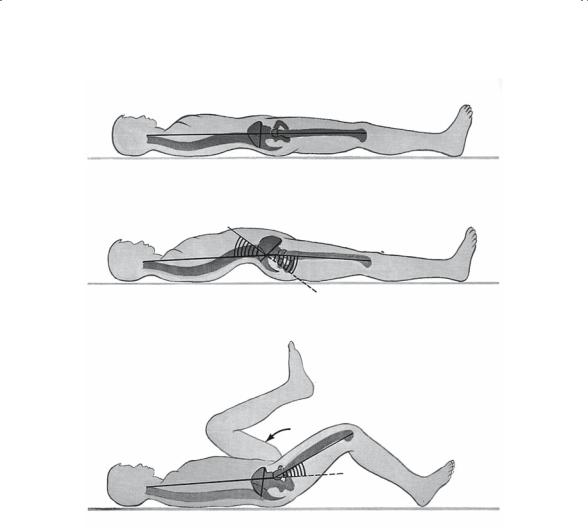
The hip should be inspected for previous scars, swelling, bruises, or abrasions. The region then should be palpated to identify areas of focal tenderness such as over the greater trochanter, sciatic nerve, or anterior hip capsule. The range of motion of the hip should then be determined. Normal range of motion of the hip is flexion to 130 degrees, extension to 20 degrees, adduction to 30 degrees, abduction to 40 degrees, internal rotation to 30 degrees, and external rotation to 70 degrees. When assessing the range of motion of the hip it is important to stabilize the lumbar spine. Motion in the lumbar spine may be attributed to the hip if the examiner is not careful. The Thomas test will stabilize the lumbar spine to measure for a flexion contracture of the hip (Fig. 11-6). Movement of the pelvis with abduction and adduction can be accurately assessed by placing a hand on the opposite anterosuperior iliac spine and recording the amount of motion before pelvic abduction.
To assess the function of the hip abductor muscles, the patient should lift the involved leg off the floor while standing. The patient should now be standing on the uninvolved leg and the pelvis should remain level. The patient now stands on the involved leg and lifts the uninvolved leg off the floor. If the pelvis is level, then the patient has normal strength of the abductor muscles. If the pelvis is noted to be lower on the elevated leg, then the abductor muscles are weak or the hip that is weight-bearing is painful. This result is referred to as the Trendelenburg sign.
A careful neurologic examination and lumbar spine examination are essential to assessing the possibility of spine pathology producing pain radiating to the hip. Patients with significant arthritic disease in the hip also commonly have spine pathology. Hip arthritis and restriction in hip range of motion can exacerbate spine pathology. The limited range of motion of the hip results in increased motion at the lumbosacral junction, which can aggravate degenerative facet arthropathy and lumbar stenosis. Replacement of the hip and improvement in the range of motion in the hip,
424 B.G. Evans
A
Normal lumbar lordosis Hip in neutral position
Normal pelvic inclination
BNote increased pelvic inclination
Compensatory lumbar lordosis in flexion contracture of the hip
C
Opposite hip and knee are maximally flexed
25°
Lumbar spine flattens Note flexion contracture of hip
FIGURE 11-6. Diagrammatic representation of the Thomas test to assess hip flexion contracture. (Adapted from von Lanz T, Wachsmith W: Praktische Anatomic. Berlin, Julius Springer, 1938, p 157.) (From Tachdjian MO: Pediatric Orthopaedics, ed 2. Philadelphia, WB Saunders Company, 1990, p 28. Reprinted by permission.)
however, can relieve stress from the lumbosacral junction and subsequently relieve the patient’s pain.
In addition, the pulses should be palpated in the foot and ankle. Significant reduction may indicate vascular insufficiency and may require further evaluation. Vascular compromise may impair wound healing or may lead to acute vascular crisis in the early postoperative period if this is not recognized and treated before any elective hip procedure. In addition, if any significant vascular reconstruction has been done in the area of the involved hip, care must be taken at the time of surgery to avoid damage to the previous reconstruction.