


Acute Severe Asthma |
86 |
|
|
Krishan Chugh |
|
A 6-year-old girl developed worsening of her asthma symptoms one early morning. Her mother administered her two puffs of salbutamol with spacer. Not seeing any improvement after 15 min, she gave her two more puffs and moved her to the neighborhood nursing home. At arrival there the pediatrician found her to be dyspnoeic, diaphoretic, and unable to talk in full sentences. Auscultation of the chest revealed B/L ronchi. Her SpO2 was 90%.
Acute severe asthma results from reversible airway obstruction mostly expiratory, with main reason of obstruction being bronchospasm due to various trigger factors (such as allergens or viral respiratory infection) and inflammation of the bronchi and smaller airways. This leads to progressive hypoxemia and hypercarbia requiring bronchodilator nebulizer therapy, systemically administered anti-inflammatory agents (steroids), and sometimes mechanical ventilation.
Step 1: Initial resuscitation
Assess airway, breathing, and circulation and take resuscitative measures as described in Chap. 78.
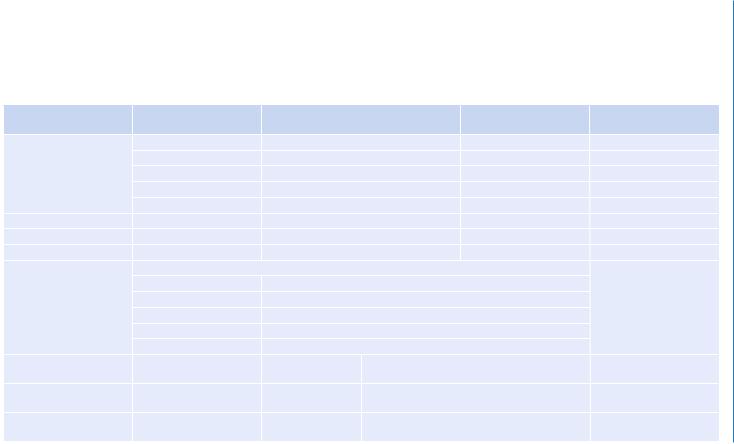
Step 2: Assess severity of the asthmatic attack (Table 86.1)
•The rapid assessment of a child with status asthmaticus should focus on determining the severity of airway obstruction.
•Wheezing, which reflects turbulent airflow in obstructed airways, is usually equally audible on both hemithoraces. Asymmetric wheezing may imply unilateral atelectasis, pneumothorax, or foreign body. Expiratory wheezing alone is
K. Chugh, M.D. (*)
Department of Pediatrics, Institute of Child Health, Sir Ganga Ram Hospital, New Delhi, India
e-mail: chughk2000@yahoo.co.in
R. Chawla and S. Todi (eds.), ICU Protocols: A stepwise approach, |
691 |
DOI 10.1007/978-81-322-0535-7_86, © Springer India 2012 |
|

694 |
K. Chugh |
|
|
found in mild-to-moderate illness, whereas expiratory plus inspiratory wheezing is present in moderate-to-severe status asthmaticus.
•The silent chest is an ominous sign and may indicate either pneumothorax or the complete absence of airflow due to severe airway obstruction and imminent respiratory failure.
•Blood gas analysis may support the clinical judgment of severity; an increasing
level of CO2 is an ominous sign. During a moderate asthma attack, a capillary blood gas analysis may be sufficient; in patients admitted to an intensive care unit, arterial blood gas analyses should be a routine. Sequential measurements are important as respiratory alkalosis with hypocarbia is common during the early phases of an asthma attack, while normalization and a subsequent increase
in the PaCO2 may be important indicators of clinical deterioration. Thus, a normal PaCO2 with even borderline low PaO2 indicates a phase of rising PaCO2, hence, need for more intensive therapy.
•A chest X-ray may be relevant in search for underlying complications such as pneumonia or air leakages.
Step 3: Review ongoing treatment
•Take into consideration the treatment that the child may have received in the past few hours. This helps us in deciding where in the treatment algorithm (Fig. 86.1) we should start. For example, in a child who has received several doses of salbutamol in the past 1 h, it may be futile to begin treatment at the top end of the algorithm.
Step 4: Start treatment (Fig. 86.1)
•Follow the algorithm for treatment.
•Generally children tolerate repeated doses of salbutamol very well and tachycardia as a side effect is less worrisome.
Step 5: Monitor closely
•At all stages, the child should be constantly monitored and escalation or deescalation of therapy should be done accordingly. For example, a child who is showing signs of exhaustion may have to be intubated straightaway even if IV b-agonist or aminophylline has not yet been tried.
Step 6: Further treatment
•Intravenous ketamine can be tried in children who are not improving on intravenous b-agonist, intravenous steroids, and supportive therapy. It is a sedative that has bronchodilator properties. Generally, it is started in the dose of 1 mg/kg/h after a loading dose of 1 mg/kg. The infusion can be increased to 3 mg/kg/h. However, all preparations should have been made for intubation and ventilation before starting IV ketamine.
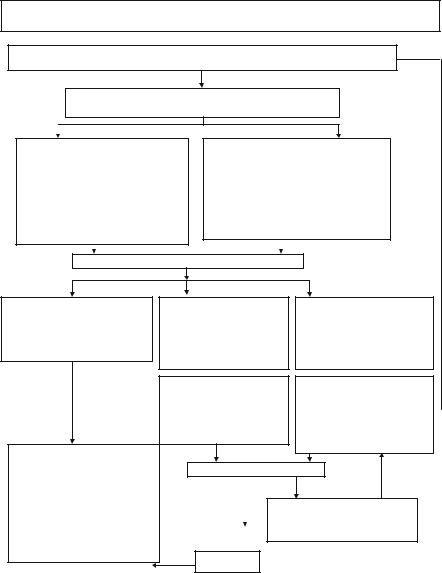
 Consider intravenous
Consider intravenous