

Status Epilepticus |
28 |
|
|
Jagarlapudi M. K. Murthy |
|
A 31-year-old female patient, with a known case of epilepsy for 10 years on irregular treatment (phenytoin 300 mg/day and clobazam 10 mg/day), was brought to the emergency department with recurrent generalized tonic–clonic seizures and not regaining consciousness for half an hour.
Status epilepticus or recurrent seizures carry a mortality as high as 30% in adults and should be managed in a systematic way.
Step 1: Initiate resuscitation
•Initial priority in an ongoing seizure patient is airway protection.
•This can be achieved by proper positioning, oral suctioning, and oral/nasopharyngeal airway devices.
•If necessary, the patient should be intubated.
•Urgent peripheral intravenous (IV) access should be established.
•Blood glucose should be checked and corrected.
Step 2: Terminate seizures
•Immediate measures should be taken to end ongoing seizure activity (Table 28.1).
•Operational definition for convulsive status epilepticus (CSE) for adults and older children (>5 years old) is “a continuous, generalized, convulsive seizure lasting more than 5 min, or two or more seizures during which the patient does not return to baseline consciousness.”
J.M.K. Murthy, M.D., D.M. (*)
Department of Neurology, The Institute of Neurological Sciences Care Hospitals, Hyderabad, India
e-mail: jmkmurthy@satyam.net.in
R. Chawla and S. Todi (eds.), ICU Protocols: A stepwise approach, |
229 |
DOI 10.1007/978-81-322-0535-7_28, © Springer India 2012 |
|
230 |
J.M.K. Murthy |
|
|
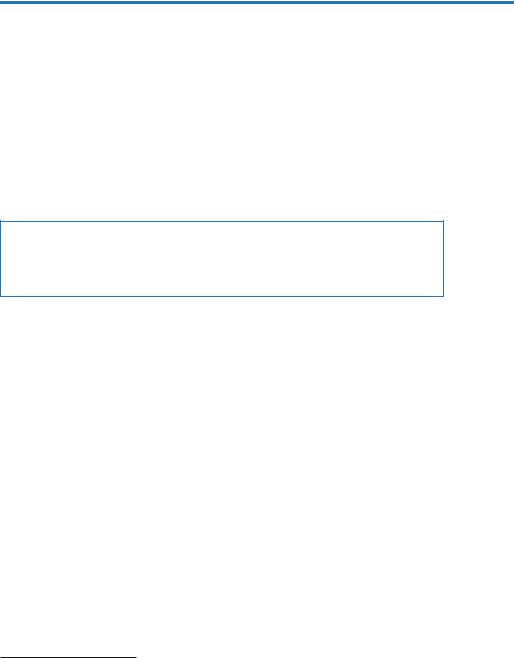
Table 28.1 Treatment algorithm for convulsive status epilepticus
I.Premonitory stage—prolonged seizures (out-of-hospital) (5 min)
•Children and young adults: Rectal diazepam 0.5 mg/kg; buccal midazolam 0.2 mg/kg
•Adults: Intravenous lorazepam 2 mg×1 or diazepam 5 mg×1, buccal midazolam 10 mg
II.First stage/out-of-hospital or in-hospital (5–20 min)
•Children and adults: Lorazepam 0.1 mg/kg IV (maximum, 4 mg) over 1 min or diazepam 0.2 mg/kg/ IV (maximum 10 mg) over 1 min. Allow 5 min to determine whether seizures terminate; if no response, repeat once
III.Second stage or established GCSE (20–60 min)
•Children and adults: Phenytoin 15–20 mg/kg IV at maximum rate of 50 mg/min or fosphenytoin 15–20 mg phenytoin equivalent (PE) IV mg/kg at maximum rate of 150 mg PE/min
If seizure continues after 10 min of phenytoin/fosphenytoin
•Repeat phenytoin 5 mg/kg IV at a maximum rate of 50 mg/min or fosphenytoin 5 mg PE/kg IV at a maximum rate of 150 mg/min or valproic acid 40–60 mg/kg IV at a maximum rate of 6 mg/kg/h or phenobarbital 20 mg/kg IV at 60 mg/min
IV. |
Refractory status epilepticus (>60 min) |
|
• Adults and children: Midazolam 0.2 mg/kg IV (maximum 10 mg) bolus over 2 min |
|
followed by 0.05–0.5 mg/kg/h cIV or propofol 2–5 mg/kg IV bolus followed by |
|
5–10 mg/kg/h cIV or thiopental 10–20 mg/kg IV bolus followed by 0.5–1 mg/kg/h |
|
cIV or pentobarbital bolus 10 mg/kg at <25 mg/min followed by cIV 0.5–2 mg/kg/h |
|
If seizures continue, consider the following emerging therapies |
|
• Topiramate 150–800 mg bid via NGT or levetiracetam 20–30 mg/kg IV at 5 mg/kg/ |
|
min (maximum 3 g) |
|
• Inhalational anesthetic agents: Isoflurane at 0.8–2 vol.%, titrated to obtain the EEG |
|
burst suppression pattern |
|
• Ketamine: 1.5 mg/kg bolus, cIV 0.01–0.05 mg/kg/h |
IV intravenous, cIV continuous intravenous infusion, NGT nasogastric tube, GCSE generalized convulsive status epilepticus
•This definition is based on the observations that spontaneous cessation of generalized convulsive seizures is unlikely after 5 min.
•For the purpose of standardization, initial pharmacotherapy of seizure has been divided into four stages (Table 28.1):
1.Premonitory stage—epileptic seizure (out-of-hospital) (5 min)
2.First stage—out-of-hospital or in-hospital (5–20 min)
3.Second stage—established status epilepticus (20–60 min)
4.Third stage—refractory status epilepticus (RSE) (>60 min)
•Benzodiazepines (lorazepam, midazolam, and diazepam) are effective in terminating seizures in 59–78% of patients. A clear benefit of IV lorazepam over diazepam has been shown in terminating CSE.
Step 3: Prevent further seizures (Table 28.1)
•When benzodiazepines fail to terminate CSE and to control further seizures once the initial seizure is controlled, a second-line drug like phenytoin or fosphenytoin is considered.

28 Status Epilepticus |
231 |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
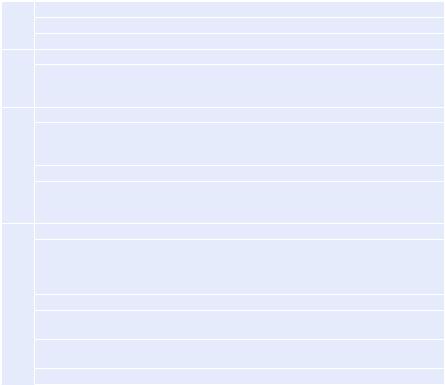
Fig. 28.1 Recurrent seizure |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Recurrent seizure |
|
|
|
|
|
|
||
management |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
ABC, 50 mL 50% dextrose, |
|
|
|
|
|
|
|
|
|
|
|
|
thiamine 100 mg IV |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lorazepam 4 mg IV; repeat 2 mg IV |
|
|
|||||||
|
|
|
|
|
after 10 minutes if needed |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phenytoin 20 mg/kg (50 mg/min) |
|
|
|
|
|
||
|
|
|
|
or Fosphenytoin dose is 15–20 mg |
|
|
|
|
||||
|
|
|
|
of phenytoin equivalent (PE)/kg at |
|
|
|
|
||||
|
|
|
|
|
100–150 mg PE/min |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Repeat phenytoin 5–10 mg/kg or fosphenytoin 5–10 |
|
|||||||||
|
|
|
|
|
PE/kg IV if seizure persists |
|
||||||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Midazolam 0.2 mg/kg IV load followed by 0.1–2.0 mg/kg/h |
|||||||||||
|
|
|
|
|
or propofol 1–2 mg/kg IV load |
|||||||
|
|
|
|
|
followed by 2–10 mg/kg/h infusion |
|||||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Continuous EEG monitoring; |
|
|
|
|
|
||
|
|
|
|
|
achieve burst suppression |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Investigate and treat |
|
|
|
||||
|
|
|
|
|
underlying cause |
|
||||||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Manage complications of |
|
|
|
|
|||
|
|
|
|
|
continuous sedation |
|
||||||
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
Taper off infusion if seizure |
|
|
|
|
|||
|
|
|
|
|
free for 24 hours |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
•Fosphenytoin is preferred to phenytoin because of its water solubility and neutral pH, thereby allowing more rapid intravenous administration with less adverse effects and its compatibility with all IV fluids.
•Phenytoin or fosphenytoin is incompatible with dextrose-containing solution.
•Phenytoin should be given through a larger vein and caution should be taken to prevent extravasation as it is highly irritant.
•Experience with IV valproic acid suggests that it is as effective as phenytoin/fosphenytoin in terminating SE in patients who have previously failed benzodiazepines and also as first-line treatment to prevent recurrent seizures (Fig. 28.1).
232 |
J.M.K. Murthy |
|
|
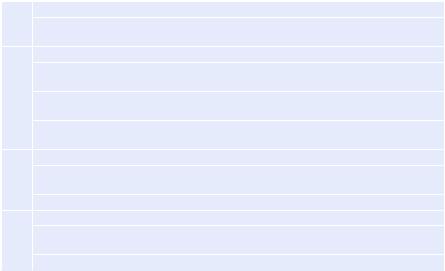
Table 28.2 Status epilepticus—general measures
I.Premonitory stage (5 min)
•Secure airway, breathing, and circulation, physical safety; check random blood glucose (glucometer)
II.First stage (5–20 min)
•Oxygen supplement; obtain IV access; stabilize airway, respiration, and hemodynamics as needed; monitor ECG and SpO2
•Thiamine 100 mg IV, 50 mL of 50% dextrose if low glucose (less than 60 mg/dL). In children younger than 2 years, pyridoxine should be added.
•Investigations: Random blood glucose, LFT, RFT, electrolytes, toxicology screening, magnesium, phosphorous, CSF if CNS infection a possibility, and CT/MRI of brain
III.Second stage or established GCSE (20–60 min)
•Cardiorespiratory function monitoring: ECG, blood pressure, SpO2; identify and treat medical complications, treat acidosis
•Investigations: EEG monitoring if the facilities are available
IV. |
Refractory status epilepticus (>60 min) |
|
|
• |
Shift to the ICU with facility for hemodynamic monitoring and cEEG monitoring, |
|
|
identification and treatment of medical complications including hyperthermia |
|
• |
Consider treating acidosis if pH 7.2 or if hemodynamically unstable |
CNS central nervous system, CSF cerebrospinal fluid, CT computer tomography, ECG electrocardiogram, EEG electroencephalogram, cEEG continuous electroencephalography, LFT liver function tests, RFT renal function tests, BUN blood urea nitrogen, MRI magnetic resonance imaging
Step 4: Initiate general measures of support and further investigation (Table 28.2)
•General supportive measures should be started concurrently with seizure treatment.
•Appropriate investigations to ascertain cause of seizures and any associated complication should also be undertaken.
Step 5: Manage refractory status epilepticus (RSE) (Table 28.1)
•Patients with refractory seizures should have their airway protected, ventilated, and hemodynamically monitored.
•Most experience is with continuous infusion (cIV) of anesthetic agents such as midazolam, propofol, and pentobarbital.
•No difference is found in mortality among the groups treated with these agents.
•Pentobarbital is associated with a lower frequency of acute treatment failures and breakthrough seizures.
•Superior pharmacokinetics and favorable adverse effect profile makes propofol a useful drug in RSE in both adults and children and successfully terminates RSE in about two-thirds of patients.
•Midazolam is an effective, short-acting benzodiazepine, which is given as an infusion, and has an efficacy in RSE.
•Studies using IV levetiracetam also suggest the efficacy and safety of the drug.