


6.4 Duplex (Duplicated) System |
189 |
|
|
•Renal and bladder ultrasound:
–This is a first-line imaging study to evaluate the upper and lower urinary tract.
–Ultrasound evaluation of upper urinary tract anomalies include ureteral duplication, dilatation of collecting system, character and thickness of the renal parenchyma.
–Ultrasound evaluation of lower urinary tract anomalies include bladder wall thickness, ureterocele, bladder diverticulum, posterior urethral dilatation, and degree of bladder emptying.
•Voiding cystourethrogram (VCUG):
–This is valuable for evaluation of the bladder and urethra.
–This includes evaluation of:
•VUR
•Bladder diverticulum
•Ureterocele
•Bladder trabeculations and bladder emptying
•Urethral anatomy during voiding
•The ureters if VUR is present
•Diuretic nuclear renography:
–This is an excellent study to evaluate:
•The differential renal function
•Cortical scars
•Drainage efficiency of the dilated collecting system based on washout times
•Intravenous pyelogram (IVP):
–This study has been largely replaced by ultrasound and nuclear renography.
–IVP delineates anatomy of the kidney, collecting system, ureter and urinary bladder.
–It also provides subjective estimation of relative renal function.
•MR urography (MRU):
–This provides excellent anatomic and functional evaluation of the renal parenchyma, collecting system and vasculature without exposure to radiation.
–MRU is sensitive to motion artifact and necessitates anesthetic sedation of young children.
•Urodynamic studies:
–This is valuable to assess voiding and bladder function in those with suspected neurogenic bladder.
•Cystoscopy, vaginoscopy, and retrograde pyelogram are endoscopic procedures that allow direct visualization of the genital and lower urinary tracts and may include radiographic visualization of the upper urinary tract (e.g. retrograde pyelogram).
•Pressure-perfusion studies (Whitaker test):
–This measure differential pressures of the renal pelvis and the bladder
–It may be useful in evaluating equivocal urinary tract obstruction
–It is invasive and depends on percutaneous placement of a catheter
–It is seldom used in the modern era of nuclear renography
6.4Duplex (Duplicated) System
6.4.1Introduction
•A duplex collecting system is one of the most common congenital urinary tract abnormalities.
•It is characterized by an incomplete fusion of upper and lower pole moieties resulting in a variety of complete or incomplete duplications of the collecting system.
•A duplex (duplicated) collecting systems can be defined as renal units containing two pyelocaliceal systems that are associated with a single ureter or with double ureters.
•The two ureters empty separately into the bladder or fuse to form a single ureteral orifice.
•Duplex collecting systems can be unilateral or bilateral and can be associated with a variety of congenital genitourinary tract abnormalities (Figs. 6.2, 6.3, 6.4, 6.5, 6.6, and 6.7).
•The exact incidence of ureteral duplication is not known but an incidence as high as 8 % in children was reported.
–Incomplete ureteral duplication was reported in approximately 1 in 25 individuals (Figs. 6.8, 6.9, 6.10, and 6.11).
–Complete ureteral duplication was reported in approximately 1 in 125 individuals (Figs. 6.12 and 6.13).

190 |
6 Congenital Ureteral Anomalies |
|
|
Figs. 6.2, 6.3, 6.4, 6.5, 6.6, and 6.7 Intravenous urography and CT urography showing duplex ureters. In the intravenous urography pictures, each ureter is draing one renal unit. There is an associated hydronephrosis in the
upper renal unit. The lower renal unit is normal. Note also on the CT urography the associated hydronephrosis and hydroureters in the lower renal unit while the upper renal unit is normal
6.4 Duplex (Duplicated) System |
191 |
|
|
INCOMPLETE OR
PARTIAL URETERAL
DUPLICATION
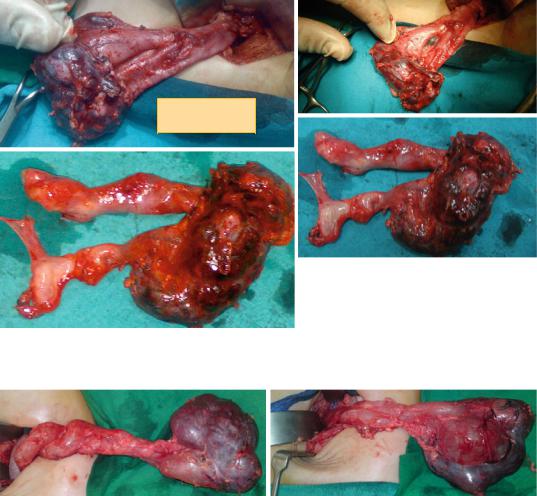
Figs. 6.8, 6.9, 6.10, and 6.11 Clinical intraoperative photographs showing duplex ureters. Note the complete and partial ureteral duplications
Figs. 6.12 and 6.13 Clinical intraoperative photographs showing complete ureteral duplication. Note the associated dysplastic kidney
• In patients with complete duplication on one |
– Complete duplication where the two ure- |
|
side, there is a 40 % chance of finding com- |
ters empty separately into the urinary |
|
plete duplication on the other side. |
bladder. |
|
• Approximately 10 % of siblings may also be |
• |
The upper ureter is more likely to be |
affected by complete duplication. |
|
associated with ectopic insertion, ure- |
• Duplex collecting systems are seen in 0.7% of |
|
terocele, and/or obstruction. |
the normal adult population and in 2–4% of |
• Caudal or medial ectopia describes the |
|
patients investigated for urinary tract symptoms. |
|
ureteral orifice when located at the |
• The duplicated ureters can be: |
|
proximal lip of the bladder neck or more |
– Bifid ureters (partial or incomplete |
|
distal. |
duplication) |
• |
The lower ureter is more frequently |
• The two ureters fuse together and insert |
|
associated with VUR. |
distally as a single ureter into the uri- |
• The upper pole is one of the components |
|
nary bladder. |
|
of the duplex kidney. |
192 |
6 Congenital Ureteral Anomalies |
|
|
•The upper pole ureter drains the upper pole of a duplex kidney.
•Similarly, the lower pole of the kidney is drained by the lower-pole ureter.
•Most patients are asymptomatic, with urinary tract abnormalities being detected incidentally on imaging studies performed for other reasons.
•These anomalies are commonly asymptomatic and considered an anatomical variant.
•Ureteropelvic obstruction is more common when a duplex kidney exists and can be inherited in an autosomal dominant pattern.
•Congenital renal anomalies in patients with classic bladder exstrophy occur in 2.8 % of patients.
•The most common anomaly is a duplicated collecting system, which occurs in approximately 1.3 % of patients.
•Duplex collecting systems may be complicated by:
–Vesicoureteral reflux
–Obstruction
–Ureterocoele
•Each of these complications may have adverse effects on the ipsilateral kidney.
•A patient’s duplex kidney is almost always more elongated than his/her nonduplex kidney.
•The kidney may be enlarged when hydronephrotic and can be associated with rotational anomalies.
•Magnetic resonance urography (MRU) may be used as the primary diagnostic method for assessing a duplex ectopic ureter, as well as the complications associated with duplex kidneys.
•If vesico-ureteral reflux exists, the presence of an ectopic ureter in a nonfunctioning moiety can best be demonstrated using a voiding cystourethrogram.
•Antegrade pyelography is useful in patients with hydronephrosis, to demonstrate the presence of a second ureter and to determine the level of ureteric termination.
•Computed tomography (CT) scanning with contrast is valuable in the evaluation of an intravesical ureterocele, either orthotopic or ectopic.
•Scintigraphy is useful in the assessment of relative renal function and in the detection of renal scars. Scintigraphy can reveal differential functioning. However, if the functioning is markedly depressed, imaging is limited.
•In the absence of obstruction and/or VUR, ureteral duplication anomalies require no specific therapy.
•Symptomatic patients usually have complete ureteric duplication in which the ureters are prone to develop obstruction, reflux, and infection.
•Duplication anomalies with associated pathology, such as VUR or obstruction, require appropriate medical therapy and possible surgical correction.
6.4.2Classification
•Duplex collecting system or duplex kidney anomalies can be classified into the following categories depending on the level or lack of fusion:
–Duplex kidney:
•The duplex kidney has a single renal parenchyma that is drained by two separate pelvicalcyeal systems
–Duplex collecting system: The kidney has two pyelocaliceal systems and is associated with a single ureter or with a bifid ureter (a partial duplication) or, in the case of a complete duplication, with two ureters (double ureters) that drain separately into the urinary bladder.
–So, a duplex collecting system is a duplex kidney draining into:
•Single ureter: Duplex kidneys and duplication pelvicalyceal systems uniting at the pelviureteric junction (PUJ)
•Bifid ureter (ureter fissus): two ureters that unite before emptying into the bladder
•Double ureter (complete duplication)
–Bifid collecting system:
•This refers to a duplex kidney with the two separate pelvicalyceal collecting systems uniting at the PUJ or as bifid ureters.