


Chapter 11 |
465 |
|
|
Infertility
Male reproductive physiology 466
Etiology and evaluation of male infertility 470
Lab investigation of male infertility 472
Oligospermia and azoospermia 476
Varicocele 478
Treatment options for male factor infertility 480

466 CHAPTER 11 Infertility
Male reproductive physiology
Hypothalamic–pituitary–testicular axis
The hypothalamus secretes luteinizing hormone–releasing hormone (LHRH), also known as gonadotrophin-releasing hormone (GnRH). This causes pulsatile release of anterior pituitary gonadotrophins, called folli- cle-stimulating hormone (FSH) and luteinizing hormone (LH), which act on the testis.
FSH stimulates the seminiferous tubules to secrete inhibin and produce sperm; LH acts on Leydig cells to produce testosterone (Fig. 11.1).
Testosterone
Testosterone is secreted by the interstitial Leydig cells, which lie adjacent to the seminiferous tubules in the testis. It promotes development of the male reproductive system and secondary sexual characteristics.
Steroidogenesis is stimulated by a cAMP-protein kinase C mechanism, which converts cholesterol to pregnenolone. Further steps in the biosynthesis pathway produce intermediary substances (dehydroepiandrosterone and androstenedione) prior to producing testosterone.
In the blood, testosterone is attached to sex hormone–binding globulin (SHBG) and albumin. At androgen-responsive target tissues, testosterone is converted into a potent androgen, dihydrotestosterone (DHT), by intracellular 5A-reductase (see p. 64).
Spermatogenesis
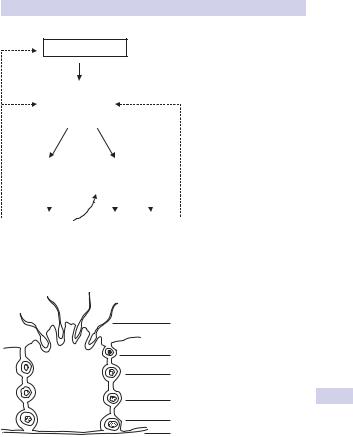
Seminiferous tubules are lined with Sertoli cells, which surround developing germ cells (spermatogonia) providing nutrients and stimulating factors, as well as secreting androgen-binding factor and inhibin (Fig. 11.2).
Primordial germ cells (spermatogonia) divide via mitosis to form primary spermatocytes. These undergo a first meiotic division to create secondary spermatocytes (46 chromosomes), followed by a second meiotic division to form spermatids (23 chromosomes). Finally, these differentiate into spermatozoa.
Spermatogenesis takes 74 days. The nonmotile spermatozoa leave the seminiferous tubules and pass to the epididymis, where they undergo maturation (gain motility and the ability to fertilized). Ductal transit time takes another 2 weeks, so the total time from beginning of spermatogenesis to ejaculation is 3 months.
Motile sperm are stored in the globus minor of the epididymis until ejaculation. Spermatozoa that are not released are reabsorbed by phagocytosis.
Mature sperm
Mature sperm have a head, middle piece, and tail (Fig. 11.3). The head is composed of a nucleus covered by an acrosome cap, containing vesicles filled with lytic enzymes that break down the outer layer of the female ovum. The middle piece contains mitochondria and contractile filaments, which extend into the tail to aid motility.
MALE REPRODUCTIVE PHYSIOLOGY 467
– ve
HYPOTHALAMUS
LHRH
– ve |
|
|
ANTERIOR |
|
|
–ve |
||
|
|
|
PITUITARY |
|
|
|
|
|
|
|
|
GLAND |
|
|
|
|
|
|
LH |
|
FSH |
|||||
|
|
|
TESTIS |
|
|
|
|
|
|
|
|
|
|
||||
Interstitial cells |
Seminiferous tubules |
|||||||
(Leydig cells) |
(Sertoli cells) |
|||||||
|
|
|
|
|
||||
|
|
|
|
|
|
|||
Testosterone |
|
Sperm Inhibin |
||||||
|
Lumen |
|
|
|
|
|
||
Figure 11.1 Hypothalamic–pituitary–testicular axis.
|
Spermatozoa |
|
Spermatid |
|
2º spermatocyte |
Sertoli cell |
1º spermatocyte |
|
|
|
Spermatogonia |
|
Basal lamina |
Figure 11.2 Spermatogenesis in the seminiferous tubules of the testis.

468 CHAPTER 11 Infertility
Head:
Plasma membrane
Acrosomal cap
Nucleus
Middle piece:
Proximal centriole
Mitochrondria
Microtubules
Tail:
Principal piece
Figure 11.3 A spermatozoon.
Tail:
End piece
After deposition at the cervix, sperm penetrate cervical mucus and travel through the uterus to the site of fertilization in the fallopian tube. Along the way, within the female reproductive tract, they undergo capacitation—a further activation of their ability to fertilize marked by an increase in their motility.
When a sperm penetrates the oocyte, it binds to the zona pellucida, which alters its permeability so that other sperm cannot penetrate the ovum, leading to enzyme release, penetration into the cytoplasm of the oocyte, fusion, and fertilization.
This page intentionally left blank