

SESSION 1
A recommendation for the future was that biodosimetry studies be combined with health outcome studies to help analyse for the existence of a possible dose response relationship.
5.IMMUNOLOGICAL EFFECTS
As with many of the effects mentioned so far, high doses of radiation can also adversely affect the function of the immune system. At low doses of radiation, the scientific literature indicates that while there may be laboratory findings there do not appear to be significant clinical changes. There are many different cell subtypes involved in mediating the immune response.
The expert group reviewed quite a number of studies of immune cell function that had been published; however, the results of the studies were often contradictory and not coherent particularly with the temporal sequence of findings. The cause of the varied effects reported was possibly felt by some of the authors to potentially be due to confounding factors (including diet, chemicals, chronic effects or radiation). Many of the Chernobyl studies were also in conflict with the detailed studies that have been performed over decades on the atomic bomb survivors. In any case, at doses of less than several tens of mGy, no clinical effects related to the immune system effects have been reported.
It was recommended that studies of the immune system continue on those exposed to high doses (more than tens of mSv) but that doses at lower dose levels would be unlikely to yield useful information. The exception to this might be children who have individually estimated doses and only when studied with appropriate control groups and a blind analysis.
6.HERITABLE, REPRODUCTIVE EFFECTS AND CHILDREN’S HEALTH
Heritable effects of radiation in humans have not been reported in the scientific literature. This does not mean that effects might not be present, but if present, they have eluded detection. Changes in fertility have been previously reported but not at doses below 0.2 Gy. Thus, heritable or fertility issues were not expected in the general population around Chernobyl. With regard to birth rate, the data is confounded by the general practice of a high rate of medical abortions that occurred both before and after the accident. Also, from the previous extensive scientific literature, congenital malformations as a result of in utero radiation were not expected at foetal doses of less than 0.1–0.2 Gy.
107
METTLER
FIG. 1. Prevalence at birth of nine types of congenital malformations in four regions (oblasts) with high and low levels of radionuclide contamination [7].
Such fetal doses were not incurred by the general population living in contaminated regions.
After reviewing the available data, the expert group concluded that there was no evidence of radiation effects on infant mortality, although quite a high rate of infant mortality compared to other countries was noted in both contaminated and non-contaminated regions. There was excellent data from Belarus on well defined congenital malformations. This data registry was in place long before the Chernobyl accident and the data show a relatively constant rise in reported congenital malformations over the period 1984–1999 [7]. Actually, the rise was similar but slightly higher in the less contaminated areas (Fig. 1). Evaluation of the incidence of Down’s syndrome in Belarus is unremarkable with the exception of a spike in January 1987 and another in May 1990 [8], which the expert group could not explain.
Infant mortality data for the year 2000 was 15 per 1000 live births in Belarus, 19 in the Russian Federation and 22 in the Ukraine compared to 10 in Poland. Data comparing infant mortality in clean and contaminated regions were only available from the Ukraine. These showed a general decrease over time, but in all areas infant mortality remains high for reasons that are unrelated to radiation exposure. There were not enough data to evaluate stillbirths and similar pregnancy complications. Several reports suggested the general health of children was decreasing for reasons other than radiation exposure. There was no evidence of hereditary effects in offspring nor would they be expected based on other scientific literature.
Recommendations included investigating the underlying cause of high infant mortality in both clean and contaminated areas, and to continue registries on reproductive health measures primarily as a public health measure and not relative to radiation effects. Actions to reduce the psychological effects
108
SESSION 1
in children and adolescents were also recommended. Studies that do not provide baseline data, the time period of observation, estimates of absorbed dose and blind evaluation of the data should be discouraged.
7.PSYCHOLOGICAL MENTAL AND NERVOUS SYSTEM EFFECTS
Data sought by the expert group included information on possible mental retardation after in utero exposure, direct effects on the brain in highly exposed individuals and psychological effects. While there were some studies on the first two topics, the series was small and the data unconvincing with little evidence of a dose response relationship, and most lacked good control groups.
The expert group agreed that psychological effects represent the largest public health impact from the accident. It was not felt to be possible to distinguish psychological effects due to the accident from other stressors occurring over the last two decades including the breakup of the Soviet Union and economic issues. It is clear that high levels of anxiety continue up to the present. There have been few studies that have integrated mental and physical health, and future studies should attempt to do this. Knowledge gaps remain with regard to systematic studies of highly exposed workers, studies of children and adolescents, and what the best interventions are to reduce anxiety.
It was concluded that serious mental problems exist but that these are at a subclinical level with implications for subjective health, reproductive health and medical service utilization. It is also clear that after future accidents some of these issues might be reduced through provision of timely and accurate information.
The group recommended that a general public health policy be generated for the population due to high rates of psychiatric and substance disorders in the population. There might also be a benefit in conducting additional research on cognitive changes in the group of acute radiation sickness survivors, hopefully with imaging or pathological correlation. There is also a need for an increase in mental health training for primary physicians and nurses, and a need to move the locus of care to primary care settings.
8.MORTALITY DUE TO THE ACCIDENT
Mortality due to the accident has been an area of intense media and public interest. The deaths which occurred due to radiation in the short term are relatively well known. Data on mortality in the liquidator population occurring from 1987 to 1998 is almost exclusively derived from the Russian
109
METTLER
1.2
1.0
SIR
0.8
1980 |
1982 |
1984 |
1986 |
1988 |
1990 |
1992 |
1994 |
1996 |
1998 |
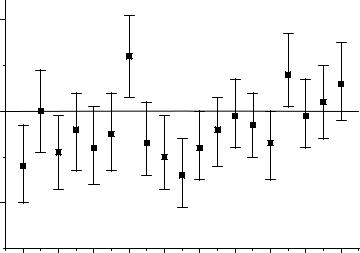
FIG. 2. All solid cancer standardized incidence ratio (SIR) among residents (both sexes) of five radioactively contaminated districts of the Bryansk region [5].
studies. Potential mortality from cancers in the future has been discussed by Dr. Cardis in her report of the 1st and 2nd meetings of the Expert Group on Health of the Chernobyl Forum [9]. The Russian liquidator studies indicate that the standardized mortality ratio (SMR) for all causes, malignant neoplasms and non-cancer diseases has been less than that of the general population (SMR < 1.0). When the liquidators are compared internally, there may be a slight excess of cancers [5]. The mortality from cardiovascular diseases was discussed earlier.
As mentioned earlier, analysis of the mortality data in the general public is confounded by the general reduction in lifespan. The death rate per 1000 in 2000 was 14 in Belarus, 15 in Russia, 16 in the Ukraine and 10 in Poland (see Table 1). When the death rate in contaminated areas of the Ukraine was examined, it averaged about 18.5 per 1000; however, these data are not age adjusted and the younger population probably has preferentially left the contaminated areas. The standardized incidence ratio (SIR) of neoplasms among the general public in contaminated districts in the Bryansk region has generally been slightly less than unity where the control was the population of other, non-affected districts of the same region (Fig. 2).
In the acute phase of the accident, there were 28 deaths due to acute radiation sickness and two deaths due to the explosion and thermal burns [4]. Another 19 acute radiation sickness patients died in 1987–2004 from various
110