


39
gross and laParoscoPic anatomy of thE UPPEr Urinary tract and rEtroPEritonEUm
Retroperitoneal Lymphatics
The retroperitoneum is rich in lymphatic structures.The lymphatic drainage of the lower extremities, perineum and external genitalia, and pelvic viscera including the lower urinary tract, must course through the retroperitoneum. The lymphatics from these large anatomic distributions eventually coalesce into the common iliac lymphatic vessels and nodes, thereafter forming ascending vertical lumbar lymphatic chains that follow the great vessels, the aorta and inferior vena cava, superiorly (see Fig. 2.1). The ascending lumbar lymphatics are closely applied to the great vessels, with multiple transverse communications between ascending lymphatic channels. It is notable that most of the lateral flow between the ascending lumbar lymphatic trunks moves from right to left. During their retroperitoneal course, these ascending lymphatic trunks are joined by the lymphatic drainage of the gastrointestinal tract, which follows the inferior mesenteric, superior mesenteric, and celiac arteries. Most, if not all, of these ascending lymphatics eventually coalesce to form the thoracic duct. In most cases, the site of this coalescence is marked by a localized dilation of the lymphatic chain which is called the cisterna chyli, usually located in a retrocrural position behind the aorta and anterior to the first or second vertebral body. It is of descriptive and practical use to distinguish three major lumbar nodal areas within the retroperitoneum: (1) the left paraaortic lymph nodes along the left lateral aspect of the aorta, (2) the right paracaval lymph nodes along the right lateral aspect of the inferior vena cava, and (3) the interaortocaval lymph nodes between the great vessels.
The retroperitoneal lymphatics are the secondary or extraregional nodal drainage for the prostate, bladder, and pelvic ureters; and represent the primary or regional nodal drainage for the abdominal ureters, kidneys, adrenal glands, and also the testes whose embryologic origins are from the upper retroperitoneum. The left testis drains primarily to the left para-aortic nodes, with significant drainage to the interaortocaval nodes, but essentially no drainage to right paracaval nodes. The right testis drains primarily to the interaortocaval nodes, with significant drainage to the right paracaval nodes, and also some early nodal metastases found in
the left para-aortic nodes. The kidneys have abundant lymphatic drainage, with usually several large lymphatic trunks traversing the renal sinus together with the renal blood vessels, joined by lymphatics from the renal pelvis and proximal ureter. From the left kidney, these lymphatic channels drain primarily into the left lateral para-aortic lymph nodes. From the right kidney these lymphatic channels drain primarily into both interaortocaval and right paracaval lymph nodes. Occasionally, some lymphatics from the right kidney may drain directly into left lateral para-aortic lymph nodes. The lymphatic drainage of the ureters generally parallels their arterial supply. The left para-aortic lymph nodes are the primary site of lymphatic drainage from the abdominal portion of the left ureter. The abdominal portion of the right ureter drains primarily to right paracaval and interaortocaval lymph nodes.
Retroperitoneal Nerves
The paired thoracolumbar symphathetic trunks arise within the chest and course vertically downward along the anterolateral aspect of the spinal column through the retroperitoneum, lying within the groove between the medial aspect of the psoas muscle and the spine bilaterally. The lumbar sympathetic trunks contain variable numbers of ganglia. Sympathetic nerve fibers supplying the abdominal viscera exit the lumbar sympathetic trunks and extend anteriorly over the aorta, forming autonomic nervous plexuses associated with the major branches of the abdominal aorta (see Figs. 2.1 and 2.2). Additional parasympathetic input to these plexuses derives from branches of the vagus nerves. The first and largest of the autonomic nervous plexuses in the abdomen is the celiac plexus on the anterior aorta surrounding the celiac artery. Through this celiac plexus passes most or all of the autonomic innervation to the adrenal, kidney, renal pelvis, and ureter. At the lower extent of the abdominal aorta,the superior hypogastric plexus lies on the aorta anterior to its bifurcation, below the takeoff of the inferior mesenteric artery, and extends inferiorly onto the anterior surface of the fifth lumbar vertebra. Much of the sympathetic input to the pelvic urinary organs and genital tract passes through this plexus. Surgical disruption of the hypogastric plexuses
40
Practical Urology: EssEntial PrinciPlEs and PracticE
Greater splanchnic n. |
|
|
Diaphragm |
Greater splanchnic n. |
|
|
||
12th rib |
Aortic hiatus |
|
|
||
Aponeurosis of |
|
|
transversus |
12th rib |
|
abdominis m. |
Sympathetic trunk |
|
Subcostal n. |
||
|
||
lliohypogastric n. |
Genitofemoral n. |
|
|
||
llioinguinal n. |
lliohypogastric n. |
|
|
||
Genitofemoral n. |
llioinguinal n. |
|
|
||
Psoas m. |
Lateral femoral |
|
cutaneous n. |
||
|
||
lliacus m. |
Obturator n. |
|
Lateral femoral cutaneous n. |
Accessory obturator n. |
|
|
||
Femoral n. |
Lumbosacral trunk |
|
Femoral branch of |
||
|
||
Genitofemoral n. |
Peritoneum |
|
Genital branch of |
||
Femoral n. |
||
Genitofemoral n. |
||
External iliac artery |
External iliac artery |
|
|
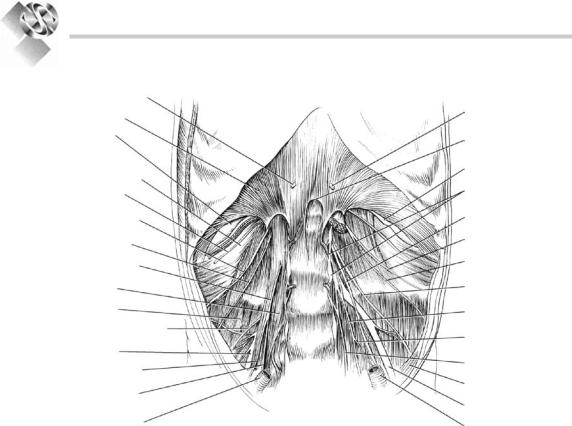
Figure 2.13. major nerves within the retroperitoneum (reprinted with permission from Kabalin1 copyright Elsevier 2002).
can cause loss of seminal vesicle emission and/ or failure of bladder neck closure that results in retrograde ejaculation.
The somatic sensory and motor innervation to the lower abdomen and lower extremities also traverses the deep retroperitoneum. The lumbosacral plexus is formed from branches of all lumbar and sacral spinal nerves. Nerves from this plexus extend through the psoas muscle (Fig. 2.13). The subcostal nerve is the anterior extension of the 12th thoracic nerve and extends forward, laterally and then anteriorly, from beneath the 12th rib. The iliohypogastric and ilioinguinal nerves originate together from the first lumbar spinal nerve. Together, these three somatic nerves provide multiple motor branches to the abdominal wall musculature, and also cutaneous sensory branches to the lower abdomen and genitalia. The lateral femoral cutaneous nerve and the genitofemoral nerve arise from the first through third lumbar spinal nerves. They provide cutaneous sensory branches to the upper thigh and genitalia. The genital branch of the genitofemoral nerve supplies motor innervation to the cremaster and dartos
muscles in the scrotum. The genitofemoral nerve lies directly on top of the psoas muscle along its retroperitoneal course and can be readily identified in this position. The femoral nerve is a much larger structure, arising from the second through fourth lumbar spinal nerves, and is largely hidden by the body of the psoas muscle in the deep retroperitoneum before exiting the abdomen lateral to the femoral artery in the groin. This important nerve supplies motor innervation of the psoas and iliacus muscles and the large muscle groups of the anterior thigh, as well as sensory branches to anteromedial portions of the lower extremity. The femoral nerve may be compressed by retractor blades placed inferolaterally against the inguinal ligament during operations on the lower abdomen and pelvis, which can produce a significant motor palsy that prevents active extension of the knee. The obturator nerve, an important lateral pelvic landmark, actually arises in the retroperitoneum from the third and fourth lumbar spinal nerves, and eventually provides motor innervation to the adductor muscles of the medial thigh.

41
gross and laParoscoPic anatomy of thE UPPEr Urinary tract and rEtroPEritonEUm
The Adrenal Glands
Although not strictly part of the urinary tract, the adrenal glands are intimately related anatomically to the kidneys and much adrenal surgery is performed by urologists. The adrenal glands are paired, yellow-orange, solid endocrine organs that lie within Gerota’s fascia superomedial to the kidneys (see Fig. 2.2). The normal adult adrenal gland weighs approximately 5 g and measures 3–5 cm in greatest dimension. The right adrenal gland assumes a pyramidal shape and rests more superior to the upper pole kidney. The left adrenal gland has a more crescentic shape and rests more medial to the upper pole of the left kidney, sometimes directly atop the left renal vein. The right adrenal thus tends to lie more superiorly in the retroperitoneum than the left adrenal, even though the right kidney, in general, lies somewhat more inferiorly than the left kidney. The right adrenal gland may also extend posterior to the inferior vena cava, making surgical access from any anterior approach more difficult.
Each adrenal is a composite of two separate and functionally distinct glandular elements: the peripheral cortex and central medulla. The medulla consists of chromaffin cells derived from the neural crest and is intimately related to the sympathetic nervous system. The adrenal medulla produces neuroactive catecholamines which are released directly into the blood stream via an extensive venous drainage system. The adrenal cortex is mesodermally derived and encases the medulla. Three separate cortical layers can be identified. Outermost is the zona glomerulosa, which produces aldosterone. Next is the zona fasciculata, which produces
glucocorticoids. The innermost layer is the zona reticularis, which produces sex steroids. The substance of the adrenal glands is inherently quite delicate and friable, and is enclosed by a collagenous capsule.
The adrenal glands are supplied by multiple small arterial branches which originate from three major arterial sources: (1) superior branches from the inferior phrenic artery on the diaphragm, (2) medial branches directly from the aorta, and (3) inferior branches from the ipsilateral renal artery. In contrast to these multiple small arterial branches, typically a single large adrenal vein drains from each gland along its anteromedial aspect. The right adrenal vein is very short and enters the inferior vena cava on its posterolateral aspect.The left adrenal vein is more elongated and often joined by the left inferior phrenic vein before entering the superior aspect of the main left renal vein. The adrenal lymphatics exit the glands along the course of the venous drainage and empty into para-aortic lymph nodes. The adrenal medulla receives greater autonomic innervation than any other organ in the body.Multiple sympathetic fibers enter each adrenal along the course of the adrenal vein to synapse with chromaffin cells in the medulla.
References
1.Kabalin JN. Surgical anatomy of the retroperitoneum, kidneys, and ureters. In: Walsh PC, Retik AB, Vaughan ED Jr, Wein AJ, eds. Campbell’s Urology. 8th ed. Philadelphia, PA: Saunders; 2002:3-40
2.Resnick MI, Parker MD. Surgical Anatomy of the Kidney. Mount Kisco, NY: Futura; 1982
3.Sampaio FJB. Renal anatomy: endourologic considerations. Urol Clin North Am. 2000;27:585-607