

Атлас по рентгенологии травмированных собак и кошек / an-atlas-of-radiology-of-the-traumatized-dog-and-cat
.pdf232 Radiology of Abdominal Trauma
Case 3.18
3
Noncontrast
Signalment/History: “Lady”, a 9-month-old, female Collie, had been hit by a truck 24 hours previously. She was in an emergency clinic being treated for shock. The BUN level and the WBC count were elevated.
Physical examination: Crepitus was detected in the pelvis. The dog had not been observed to urinate since the accident and the bladder could not be identified by palpation.
Radiographic procedure: Only lateral radiographs were made of the abdomen and pelvis because of the severity of the injuries.
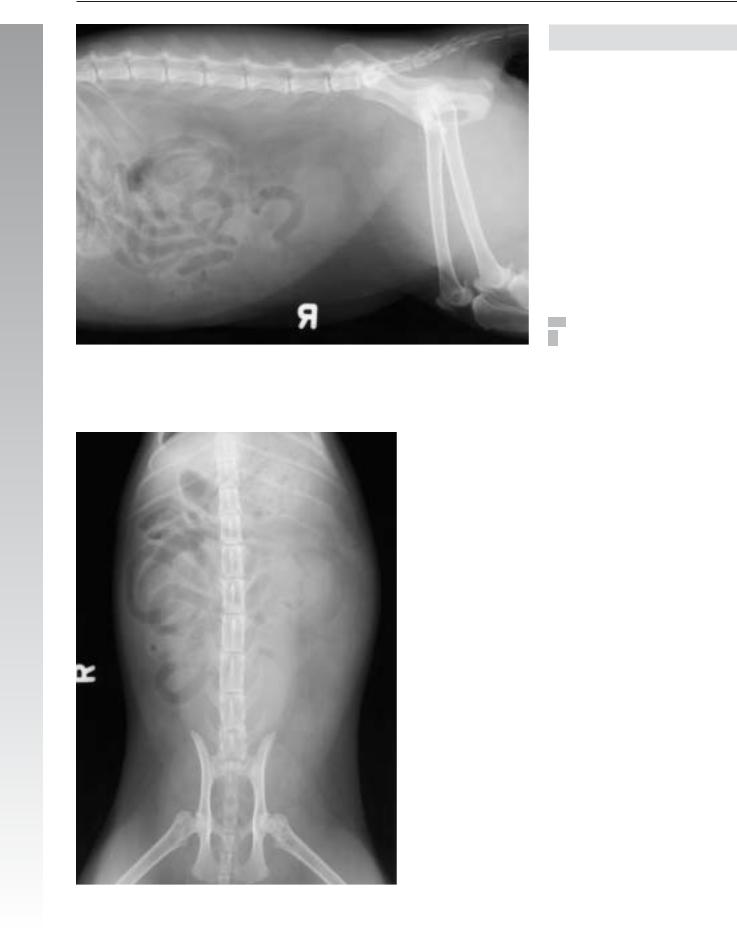
Radiographic diagnosis: Marked gaseous distention of small bowel loops in the midabdominal region suggested a paralytic ileus. Loss of contrast between the abdominal viscera, failure to clearly identify the urinary bladder, and failure to identify the ventral abdominal wall all indicated free peritoneal fluid. Small air pockets throughout the abdomen suggested the presence of free peritoneal air, too. Retroperitoneal fluid indicated possible hemorrhage. An indistinct fluid-den- sity inguinal mass was also thought to be probably due to free hemorrhage.
Treatment/Management: The small cardiac silhouette and small pulmonary vessels were noted radiographically to increase in size following administration of IV fluids. During this time, the urinary bladder was noted to remain constant in size suggesting that urine was leaking from the bladder. It was decided that an excretory urogram was necessary.
Radiographic diagnosis (10 minutes following intravenous injection): Leakage of radiopaque contrast medium in both the peritoneal and retroperitoneal spaces was suggestive of a ruptured bladder neck and/or a torn ureterovesical junction (arrows).
Treatment/Management: The paralytic ileus could have been the result of the trauma indicating injury to the vascular supply, mesenteric torsion, or herniation through a mesenteric tear. In addition, it could have been the response to urine within the peritoneal cavity. The dog was euthanized and the body taken home without any further examination.

Renal, ureteral, and urinary bladder injury 233
3
Excretory urogram

234 Radiology of Abdominal Trauma
Case 3.19
3
Signalment/History: An adult male cat had been found by the road unable to move and was brought to the clinic.
Physical examination: The patient was dyspneic and an inguinal hernia was palpated.
Radiographic procedure: Thoracic and abdominal studies were made.
Radiographic diagnosis (thorax): A massive pneumothorax had caused the collapse of the right lobes and a mediastinal shift to the left. Pulmonary contusion had induced an increase in fluid density in the left lung. An injury to the right thoracic wall had fractured a number of ribs. Minimal subcutaneous emphysema was present. The diaphragm appeared intact.
Radiographic diagnosis (abdomen): The urinary bladder appeared within an inguinal hernia on the left, which also contained air-filled small bowel loops. A right-sided pelvic fracture included injury to the floor of the pelvis, but did not affect the hip joint. Stress aerophagia resulted in the stomach being distended with air.

Renal, ureteral, and urinary bladder injury 235
3
Retrograde cystogram
Radiographic diagnosis (retrograde cystogram): The retrograde study showed the catheter tip lying within the urethra and a flow of contrast agent into the peritoneal cavity and into the hernial sac. This extra-vesicular flow of the contrast agent and the failure to fill the bladder with the agent suggested a rupture of the urethra or bladder neck. The bladder was thought to be within the hernial sac.
Treatment/Management: The cat was euthanized and the necropsy confirmed the radiographic findings of a bladder neck tear.

236 Radiology of Abdominal Trauma
Case 3.20
3
Noncontrast
Signalment/History: “King” was an 8-year-old, male Collie with a suddenly appearing caudal mass. The owners suspected that the dog had been struck by a car several weeks earlier.
Physical examination:The mass was soft and fluid-filled, but not painful on palpation. Both hip joints had limited motion.
Radiographic procedure: Both views were made of the abdomen and of the pelvis. In addition, both intravenous urography and retrograde cystography were performed.
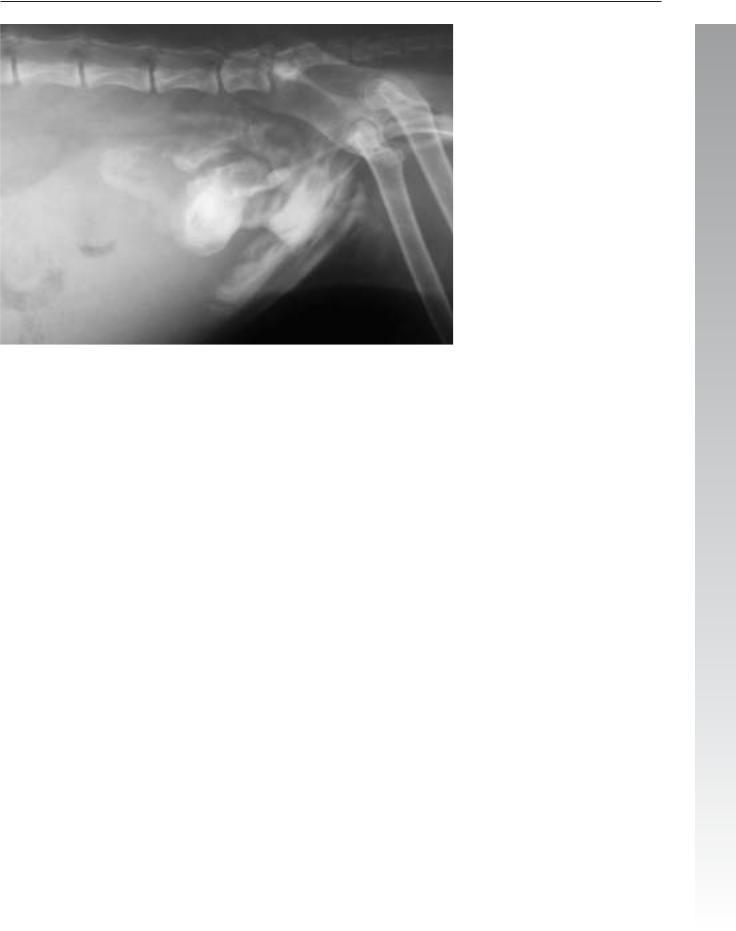
Radiographic diagnosis (noncontrast): A poorly marginated, soft tissue mass of uniform fluid density lay ventral to the tail causing the gas-filled rectum to be displaced dorsally (arrows).
Malunion pelvic fractures had caused a marked stenosis of the pelvic canal. The hip joints were difficult to evaluate.
A healed caudal sacral fracture had induced a dorsal displacement of the distal fragment.
Radiographic diagnosis (intravenous urography/retrograde cystography): A bilateral hydronephrosis and hydroureter was more prominent on the left on the ten-minute study. The trauma had caused a displacement of the urinary bladder and prostate gland into the perineal hernia. A urethral catheter positioned into the urinary bladder could be identified on the study.

Renal, ureteral, and urinary bladder injury 237
3
Retrograde cystography
Bilateral retention of the contrast agent in the pelvis and ureters following the intravenous injection was evident on the 10-minute study. On the 30-minute study, drainage had occurred from the right kidney and ureter; however, retention of contrast agent persisted on the left side (arrows).
Comments: It is interesting to speculate whether the retroflexion of the bladder had occurred at the time of the trauma that caused the pelvic fractures or was secondary to chronic straining in the months following the fractures. The owners were correct in that the dog had been traumatized; however, the trauma probably had been several months previously and not weeks as they had thought.
In the evaluation of the pelvic trauma, the status of the femoral heads is important since their injury causes a major complication to treatment and healing, as well as the ultimate prognosis. In this patient, the femoral heads and necks appear not to be traumatized. In comparison, the collapse of the pelvic inlet is important clinically.
It was possible to correct the location of the abdominal organs surgically, but little could be done concerning the malunion fractures or injury to the acetabula.

238 Radiology of Abdominal Trauma
Case 3.21
3
Signalment/History: A male DSH cat was found lying by the side of the highway apparently having been struck by a car.
Radiographic procedure: Whole body radiographs were made, followed by a retrograde cystogram.
Radiographic diagnosis (abdomen): Small bowel loops were “floating” within an abdomen without contrast and so the latter was thought to contain peritoneal fluid. The urinary bladder could not be identified.
Renal, ureteral, and urinary bladder injury 239
3
Retrograde cystogram
Radiographic diagnosis (retrograde cystogram): The positive contrast agent partially filled the urinary bladder; however, a large portion of the contrast agent spilled into the retroperitoneal cavity, peritoneal cavity, and extended into the pelvic cavity.
Outcome: At necropsy, a 1–2 cm tear was located just cranial to the trigone region of the urinary bladder. A tear in this location had permitted urine to escape into all of the adjacent body cavities. Splenic rupture with hemoperitoneum was also noted.
240 Radiology of Abdominal Trauma
Case 3.22
3
Noncontrast
Signalment/History: “Ollie” was a 2-year-old, male DSH cat with clinical signs of urinary obstruction.
Physical examination: On palpation, the urinary bladder was difficult to feel and the abdomen felt somewhat distended. During the examination, a catheter was passed into the bladder, but only a small amount of sanguinous fluid could be removed.
Radiographic procedure: Noncontrast studies were made of the abdomen and were followed by a retrograde cystogram.
Radiographic diagnosis (noncontrast): A fluid density mass was located in the caudal abdomen ventrally, but in a location thought cranial to the expected location of the urinary bladder. Bowel loops were air-filled and appear to “float” on a “sea” of peritoneal fluid, possibly urine. Loss of peritoneal contrast further supported the diagnosis of peritoneal fluid. Free peritoneal air was difficult to identify, but a large air dense shadow was noted in the midabdomen dorsally on the lateral view, and on the left side of the abdomen on the VD view.

Renal, ureteral, and urinary bladder injury 241
3
Retrograde cystogram
Radiographic diagnosis (retrograde cystogram): A small amount of positive contrast agent was injected through the catheter with the agent passing directly into the peritoneal cavity ventrally and to the right. The shadow thought to be the urinary bladder did not fill with any of the contrast agent.
Treatment/Management: The owner refused treatment. At necropsy, the catheter was found to have passed through an opening in the urethra located 3 mm from the bladder neck. The tip of the catheter was 4 cm beyond the urethral rupture into the peritoneal cavity at the time of injection. The appearance of the urethral tear suggested a chronic lesion possibly following an earlier effort at catheter placement.
While the study confirmed an injury, placement of the catheter tip within the urethra would have been more informative and would have demonstrated a lesion that could have been more easily repaired than was originally thought.