

Атлас по рентгенологии травмированных собак и кошек / an-atlas-of-radiology-of-the-traumatized-dog-and-cat
.pdf152 Radiology of Thoracic Trauma
Case 2.74
2
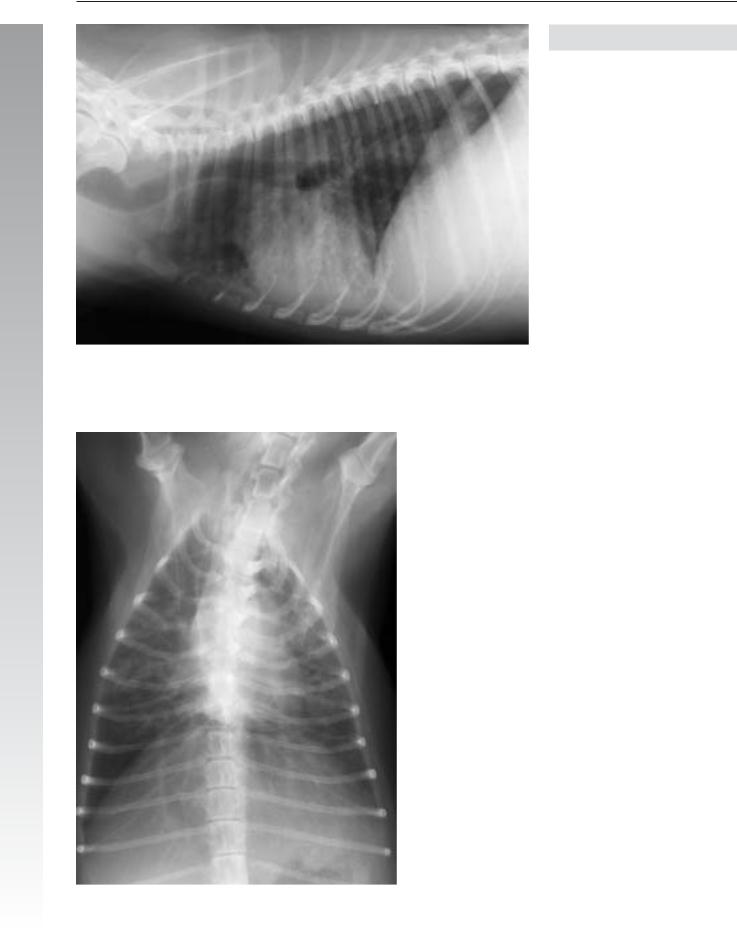
Day 1
Signalment/History: “Ming” was an 8-month-old, female Pekingese who had experienced difficulty swallowing a piece of meat, and had choked and collapsed. The owner removed the meat from the dog’s oropharynx and began cardiopulmonary resuscitation.
Physical examination: When presented to the clinic, “Ming” was alert, exhibited open-mouth breathing and had marked bronchovesicular sounds bilaterally.
Radiographic procedure: The thorax was radiographed.
Radiographic diagnosis (day 1): A generalized increase in pulmonary density was evident throughout the lung fields with a minimal air-bronchogram pattern. The diaphragm was located caudally and flattened, suggesting obstructive emphysema. The cranial mediastinum was widened, but this was thought to be breed dependent.

Iatrogenic injury 153
2
Day 2
Radiographic diagnosis (day 2): A persistent increase in pulmonary density in the left lung strongly suggested pneumonia.
Treatment/Management: It was thought that because of the small size of the dog, the resuscitation had caused trauma to the thorax and that the changes within the lung lobes represented pulmonary hemorrhage. It was also possible that small portions of food had been aspirated and so the lung changes could have been due to aspiration pneumonia. In addition, an obstructive component may have been present causing an associated obstructive atelectasis
The slow clearing of the pulmonary density plus the increase in density in the left lung on the second day both suggested the development of a secondary airway-oriented pneumonia. A simple transudate secondary to trauma should have cleared more quickly. The dog was discharged after a short stay in the clinic.
154 Radiology of Thoracic Trauma
Case 2.75
2
Signalment/History: A 12-year-old, female Beagle belonging to a colony was subjected to anesthesia for a dental procedure. Following recovery, the dog was put into a cage for the night. The next day, the dog was depressed and did not respond to stimuli.
Radiographic procedure: The thorax was radiographed.
Radiographic diagnosis: Patchy pulmonary fluid was seen in all the lobes, though it was more severe ventrally. Air-bron- chogram patterns were noted peripherally. No pleural fluid was noted. The trachea was dilated. The thoracic cavity was expanded.
Treatment/Management: The dog died shortly after the radiographs were made and was found at necropsy to have a generalized, acute aspiration bronchopneumonia secondary to aspirated vomitus.

Iatrogenic injury 155
Case 2.76
2
Signalment/History: “Zazzie” was a 15-year-old, female Poodle that had been given anesthesia for a dental extraction and had experienced a prolonged recovery. During this time, manual inflation of the lungs was performed several times. At presentation, she was awake but had difficulty in breathing.
Radiographic procedure: Radiographs were made to determine the cause of the dyspnea.
Radiographic diagnosis: A bilateral pneumothorax was associated with atelectic lungs, which included radiolucent cysts (pneumatoceles). No pleural fluid was noted. The chest cavity was expanded with the ribs at right angles to the spine. The cardiac silhouette was separated from sternum due to the pneumothorax.
Treatment/Management: The excessive pulmonary pressure as a result of the “bagging” during anesthesia could have resulted in rupture of pulmonary bullae causing the pneumothorax. These bullae may have been developmental or secondary to chronic emphysema.
It is remarkable that “Zazzie”, after recovery, was admitted to the clinic two months later with severe dyspnea and a tension pneumothorax. She underwent cardiac arrest and died. On necropsy, the lungs were atelectic, but in a randomly irregular manner because of the interposed pulmonary cysts, which were thought to be developmental.

156 Radiology of Thoracic Trauma
Case 2.77
2
Day 1
Signalment/History: “Codie”, a 2-year-old, female German Shepherd, developed a sudden onset of dyspnea and a suspicion of trauma.
Physical examination: Because of the dyspnea, the thorax was radiographed immediately.
Radiographic diagnosis (day 1): Extensive pulmonary fluid caused prominent air bronchograms in the middle lobes. The etiology could not be elucidated from the radiograph; however, a dilated esophagus depressed the air-filled trachea and indicating the possibility of an aspiration pneumonia. Note that the pulmonary lesions are only clearly identifiable on the DV view. It is possible, but unusual for an airwayoriented pneumonia to have a bilateral symmetry such as in this case.
Treatment/Management: “Codie” was treated for pneumonia. She was operated on five days later for a suspected intussusception detected on palpation as an abdominal mass without any additional thoracic radiographs being made.

Iatrogenic injury 157
2
Day 6
Radiographic diagnosis (day 6): Radiographs made postoperatively showed a marked progression of the pulmonary lesions with the left caudal lobe being the only near-normal lobe. The remaining lobes had an increased fluid content with a prominent air-bronchogram pattern. Silhouetting with the heart shadow reflected the amount of fluid content in the lungs. The dilated esophagus remained evident and continued to depress the air-filled trachea.
Outcome: The dog subsequently died. At necropsy, esophageal dilatation plus a secondary inhalation pneumonia were found. The abdominal exploratory surgery added stress to the dog and also positioned it in dorsal recumbency for several hours, probably adding to the flow of the acid-rich gastric fluids into the lungs.
Comments: Several errors had possibly been made in the handling of this patient. First, the importance of the distended, air-filled esophagus present on the first radiographs was not appreciated. Second, a second set of pre-operative radiographs was not made due to the assumption that the status of the lungs would remain static. When radiographs were made post-operatively, the progression of what was then assumed to be aspiration pneumonia was evident.

158 Radiology of Thoracic Trauma
Case 2.78
2
Referral
Signalment/History: “Fluffy”, a 2-year-old, male DLH cat, was presented with a history of gagging and regurgitation of undigested food. If fed liquids, he did not vomit. These findings followed an earlier clinic stay lasting three weeks that had been required to correct a urinary blockage. He had been anesthetized during that hospitalization.
Radiographic procedure: Thoracic studies were made with liquid barium and barium mixed with kibble (dried cat food).
Radiographic diagnosis: The liquid swallow revealed a small esophageal stricture at the level of C4 (referral and liquid barium swallow, arrow). The kibble meal allowed a more thorough understanding of the stricture (arrow).
Treatment/Management: The stricture was thought to be due to an esophagitis as a result of regurgitation during recovery from the anesthesia.

Iatrogenic injury 159
2
Liquid barium swallow
Barium swallow mixed with kibble

160 Radiology of Thoracic Trauma
Case 2.79
2
Noncontrast
Signalment/History: “Shampoo” was a 10-year-old, male Labrador Retriever mixed breed with a chronic history of dysphagia and regurgitation. He ate only blended food and could only do that successfully if the food was placed in an elevated position. The clinical problem had started some days following abdominal surgery.
Radiographic procedure: Thoracic radiographs were made followed by contrast studies using only a liquid barium meal.
Radiographic diagnosis: An air-filled dilated esophagus extended from the thoracic inlet to the carina, and appeared to be “wrapped-around” the trachea (arrows). The mediastinum did not appear to be increased in size. The lungs appeared normal.
The bolus of barium sulfate showed a persistent proximal esophageal dilatation with a failure to pass an apparent stricture at the heart base. A portion of the more liquid swallow passed the constricted segment and flowed into the caudal portion of the esophagus. The mucosal surface appeared roughened. The exact nature of the esophageal lesion was not evident on these studies.

Iatrogenic injury 161
2
Contrast
Treatment/Management: Endoscopy was limited to the cranial portion of the esophagus where granular-type lesions could be identified within the wall. Fibrotic-like tissue extended across the esophageal lumen and appeared to act as strictures. Examination of tissue removed by biopsy was con-
sistent with that resulting from a chronic esophagitis. The clinical history suggested that the injury to the esophagus could have been secondary to regurgitation at the time of the surgery.