

Appendices |
843 |
|
|
Appendix B
Common ICU Formulae
A.Pulmonary equations
1.Arterial oxygen tension (PaO2)
On room air = 100 − 1/3 (age)
On supplemental oxygen = FiO2 (in decimals) × 500, Room air FiO2 = 21% (0.21), FiO2 increases by approximately 4% for each litre increase in Supplemental Oxygen
2.Alveolar gas equation
|
|
æ PaCO2 ö |
||
|
PAO2 |
= (FiO2 ´[Patm - PH2O]) - ç |
|
÷ |
|
|
|||
|
|
è R |
ø |
|
|
PAO2 |
= 150 – (1.25 × PaCO2) |
|
|
|
Normal = 100 mmHg (room air, at sea level) |
|
||
|
where PAO2 = alveolar partial pressure of oxygen |
|||
|
FiO2 = fraction of inspired oxygen (in decimals) |
|||
|
Patm = barometric pressure (760 mmHg at sea level) |
|||
|
PH2O = water vapor pressure (47 mmHg at normal body temperature 37°C) |
|||
|
PaCO2 = partial pressure of carbon dioxide in the blood |
|||
|
R = respiratory quotient, assumed to be 0.8 |
|
||
3. |
AlveolarÐarterial oxygen gradient |
|
||
|
PAO2 − PaO2 |
|
||
|
A-a gradient (on room air) = 2.5 + 0.21 × age in years |
|||
|
Normal value = 3–15 mmHg |
|
||
|
Varies with FiO2 |
|
||
|
For FiO2 = 21%; A-a gradient = 5–15 mmHg |
|||
4. |
For FiO2 = 100%; A-a gradient = <150 mmHg |
|||
PaO2/FiO2 ratio |
|
|||
Normal = 300–500 mmHg
<300 = acute lung injury (previous definition) <200 = ARDS (previous definition)
Berlin definition:
200–300 (with PEEP/CPAP >5) = Mild ARDS <200 (with PEEP >5) = Moderate ARDS <100 (With PEEP >5) = Severe ARDS
5.ArteriolarÐalveolar oxygen ratio = PaO2/PAO2
Normal = 0.77–0.82 (most reliable when FiO2 <0.5)
6.Oxygenation index =
é |
FiO |
2(fraction of inspired O2) |
ù |
êmean airway pressure (cm H2O) ´ |
|
ú ´ 100, |
|
|
PaO2(mm Hg) |
||
ê |
|
ú |
|
ë |
|
|
û |
0 - 25= Good outcome |
|
|
|
>25–40 = severe hypoxemia |
|
|
|
844 |
Appendices |
|
|
7. Static lung compliance (Crs stat)
Tidal volume
Compliancestatic = Plateau pressure - PEEP(positive end - expiratory pressure)
Normal compliance in an intubated patient = 57–85 mL/cm H2O 8. Dynamic lung compliance (Crs dynamic)
Tidal volume
Compliancedynamic = Peek pressure - PEEP(positive end - expiratory pressure)
Variable depending on peak pressure in an intubated patient Lung + Thoracic wall compliance = 0.1 L (100 ml)/cm H2O
9. Airway resistance
Airway resistance = Peak inspiratory pressure - plateau pressure Peak inspiratory flow
Normal resistance in an intubated patient is 4–6 cm H2O/L/s
10.PaCO2–PetCO2 gradient
Normal = 4–5 mmHg
11.Dead space ventilation VD = PaCO2 - PetCO2
VT PaCO2
VD = Dead Space Ventilation = 1ml/lb (2.2 kg) of ideal body wt =150 ml VT = Tidal Volume
PetCO2 = end-tidal CO2 measured by capnography
Normal VD /VT = 0.5 (50%) in mechanically ventilated patients
0.3(30%) in spontaneously breathing patients
12.Shunt equation (right to left shunt) Qs / Qt = (CcO2 - CaO2 )
(CcO2 - CvO2 )
Qs/Qt = shunt fraction
CcO2 is the end-capillary oxygen content (estimated from the PAO2) CaO2 is the arterial oxygen content
CvO2 is the mixed venous oxygen content Normal = 5%
Alternate equation (in patients breathing 100% oxygen for 20 min)
Qs / Qt = 100 ´ (0.0031´ AaG)/ ((.0031´ AaG)+ 5)
13. PaO2 + PaCO2 <150 mmHg at sea level breathing room air
Appendices |
845 |
|
|
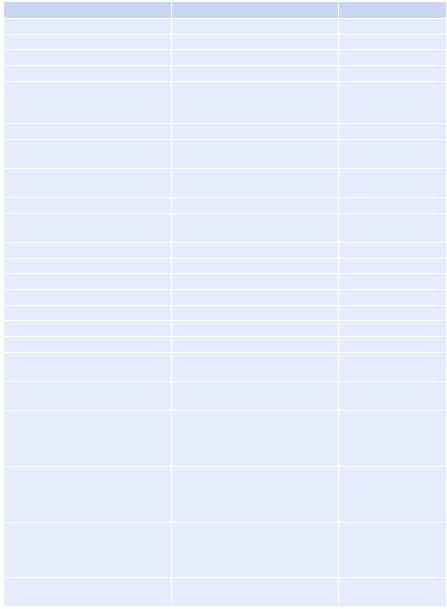
B.Hemodynamic equations
(See Chap. 16)
Parameter |
|
|
Formula |
|
|
Normal range |
||
Pulse pressure |
|
|
Systolic − diastolic BP |
40 mmHg |
||||
Mean arterial pressure (MAP) |
|
1/3 pulse pressure + diastolic BP |
65 mmHg |
|||||
Cardiac output (CO) |
|
|
SV × HR |
|
|
4–7 L/min |
||
Cardiac index (CI) |
|
|
CO/BSA |
|
|
3.5–4.5 L/min/m2 |
||
Stroke volume (SV) |
|
|
CO/HR × 1,000 End diastolic |
60–80 mL |
||||
|
|
|
volume (EDV) (120 ml) – End |
|
||||
|
|
|
systolic volume (ESV) (50 ml) |
|
||||
Stroke volume index (SVI) |
|
|
CI/HR × 1,000, SV/BSA |
33–47 mL/m2/beat |
||||
Systemic vascular resistance |
|
|
[(MAP − CVP)/CO] × 80 |
900–1,200 dyn.s/cm5 |
||||
(SVR) |
|
|
|
|
|
|
|
|
Systemic vascular resistance index |
(MAP – CVP) 80/CI |
1,970–2,390 dyn.s/ |
||||||
(SVRI) |
|
|
|
|
|
|
|
cm5/m2 |
Pulmonary vascular resistance |
|
[(MPAP − PAOP)/CO] × 80 |
80–120 dyn.s/cm5 |
|||||
Pulmonary vascular resistance |
|
[(MPAP − PAOP)/CI] × 80 |
255–285 dyn.s/cm5/m2 |
|||||
index |
|
|
|
|
|
|
|
|
Oxygen delivery (DO2) |
|
|
CO (L) × CaO2 (ml/dl) × 10 |
700–1,400 mL/min |
||||
Oxygen delivery index (DO |
I) |
|
CaO |
2 |
× CI × 10 |
|
500–600 mL/min/m2 |
|
2 |
|
|
|
|
|
|
|
|
Oxygen consumption (VO2) |
|
|
CO (L) × (CaO2 − CvO2) × 10 |
180–280 mL/min |
||||
Oxygen consumption index (VO |
I) |
CI × (CaO |
− CvO |
) × 10 |
120–160 mL/min/m2 |
|||
|
2 |
|
|
|
2 |
2 |
|
|
Oxygen extraction ratio (O2ER) |
|
VO2/DO2 × 100 |
|
25% |
||||
Oxygen extraction index (O2EI) |
|
[(SaO2 − SvO2)/SaO2] × 100 |
20–25% |
|||||
Arterial oxygen content (CaO2) |
|
(1.39 × Hb SaO2) + (0.003 × PaO2) |
17–20 mL/dL |
|||||
Mixed venous oxygen content |
|
(1.39 × Hb × SvO2) + (0.003 × |
12–15 mL/dL |
|||||
(CvO2) |
|
|
PvO2) |
|
|
|
||
A-V oxygen content difference |
|
CaO2 − CvO2 |
|
4–6 mL/dL |
||||
(C(a-v)O2) |
|
|
|
|
|
|
|
|
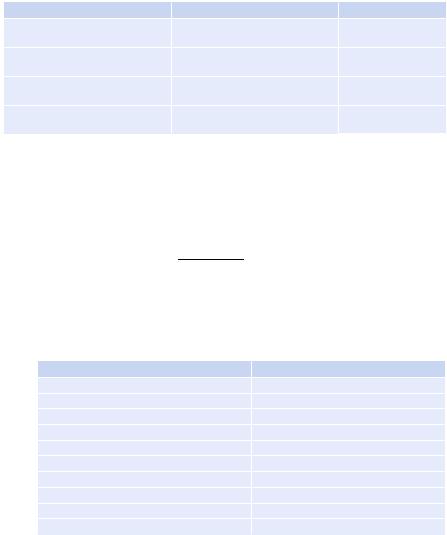
Systolic pressure variation (SPV) |
[(SPmax − SPmin)/ |
<5 mmHg unlikely to |
||||||
|
|
|
(SPmax + SPmin)/2] × 100 |
be preload responsive |
||||
|
|
|
|
|
|
|
|
>5 mmHg likely to |
|
|
|
|
|
|
|
|
be preload responsive |
Pulse pressure variation (PPV) |
|
(SVmax − SVmin)/ |
<10% unlikely to be |
|||||
|
|
|
[(SVmax + SVmin)/2] × 100 |
preload responsive |
||||
|
|
|
|
|
|
|
|
>13–15% likely to be |
|
|
|
|
|
|
|
|
preload responsive |
Stroke volume variation (SVV) |
|
SV × (MAP − PAWP) × 0.0136 |
<10% unlikely to be |
|||||
|
|
|
|
|
|
|
|
preload responsive |
|
|
|
|
|
|
|
|
>13–15% likely to be |
|
|
|
|
|
|
|
|
preload responsive |
Left ventricular stroke work |
|
|
SVI × (MAP − PAWP) × 0.0136 |
58–104 g m/beat |
||||
(LVSW) |
|
|
|
|
|
|
|
|
Appendices |
847 |
|
|
3.Metabolic acidosis
•Predicted PaCO2 = 1. 5 × [HCO3− + 8] ±2
•Change in bicarbonate = change in standard base excess (SBE)
•1 mEq/L fall in HCO3 = 1.2 mmHg fall in PaCO2
•Bicarbonate deficit (mEq/L) = [0.5 × body weight (kg) × (24 − [HCO3−])] Rule of thumb: Expected PaCO2 = the last two digits of pH after decimal
4.Metabolic alkalosis
•Predicted PaCO2 = 0.7 × [HCO3 + 21] ± 2
•Change in bicarbonate = 0.6 × standard base excess (SBE)
•1 mEq/L rise in HCO3 = 0.7 mmHg rise in PaCO2
•Bicarbonate excess [0.4 × body weight (kg) × ([HCO3−] − 24)]
Rule of thumb: Expected PaCO2 = the last two digits of pH after decimal
5.Blood anion gap
•Anion gap (AG) = Na+ − (Cl− + HCO3−)
– Normal value: 10 ± 4 mmol/L
•Correction for albumin: For every change (increased or decreased) of 1 g/dL in albumin, a change of 2.5 mmol/L in the anion gap
•Correction for pH: In acidosis, decrease by 2 mmol/L; in alkalosis, increase by 2 mmol/L
6.Delta gap/Delta ratio
•Delta gap = delta AG − delta HCO3−
•Delta ratio = delta AG/delta HCO3
•Where Delta AG = patient’s AG − 12 mEq/L {normal AG}
•Delta HCO3− = 24 mEq/L {normal HCO3−} − patient’s HCO3
• Normal delta gap (in pure anion gap metabolic acidosis) = 0 ± 6
•Normal delta ratio =1.1
–High delta gap/delta ratio > 1 signifies a concomitant metabolic alkalosis or chronic respiratory acidosis.
–Low delta gap/delta ratio < 1 signifies a concomitant normal anion gap metabolic acidosis or chronic respiratory alkalosis.
7.Urine anion gap (UAG)
•UAG (mmol/L) = urine [(Na + K) − Cl]
–Normal: usually zero or positive
–Nonanion gap metabolic acidosis due to gastrointestinal loss: UAG negative
–Nonanion gap metabolic acidosis due to renal cause (renal tubular acidosis): UAG positive
8.Stewarts approach
•Strong ion difference (SID): [Na+]+[K+]+[Ca2+]+[Mg2+]−[Cl−]−[lactate]
–Normal value: 40 mEq/L
–Increase in SID = alkalosis (increase in pH)
–Decrease in SID = acidosis (decrease in pH)
•Strong ion gap (SIG): SID − SIDeff
–SIDeff = effective strong ion difference (depends on pH, albumin, phosphate)
848 |
Appendices |
|
|
–12.2×PCO2/(10 − pH) + [albumin] × (0.123 × pH − 0.631) + [PO4−] × (0.3 09 × pH − 0.469)
–Normal SIG = 0
–Positive SIG = Increase in organic acid D. Electrolyte equations
1.Hyponatremia
•Sodium deficit = (desired [Na+] − current [Na+]) × 0.6 × body weight in kg
•Increase in serum sodium = (infusate sodium − serum sodium)/[(0.6 × body weight) + 1]
Rule of thumb:
–For hypertonic (3%) saline, infusion rate (mL/h) = weight (kg) × desired rate of correction (mEq/h)
–e.g. to correct sodium by 0.5 meq/l/hr, the desired rate of 3% saline infusion in a 60 kg man would be = 60 × 0.5 = 30 ml/hr
–0.9% NaCl corrects at 1–2 mmol/L for every 1 L NaCl
•Calculated urine osmolarity=the last two digits of urine-specific gravity×30
2.Hypernatremia
|
æ plasmaNa+ |
ö |
||
• |
Free water deficit (L) = 0.4 ´ body weight ´ ç |
|
-1÷ |
|
140 |
||||
|
è |
ø |
||
3.Correction sodium for hyperglycemia
•For each 100 mg/dL increase in blood glucose above 200 mg/dL, serum sodium decreases by 2.4 mEq/L.
4.Serum osmolality
•Calculated Sosm = (2 × serum [Na]) + [glucose, in mg/dL]/18 + [blood urea nitrogen, in mg/dL]/2.8
•Calculated Sosm with standard units (mmol/L) = (2 × serum [Na]) + [glucose] + [urea]
–Normal value = 270 and 290 mOsm/kg H2O
•Osmolar gap = measured osmolality − calculated osmolality
–Normal value = <10 mOsm/kg H2O
5.Corrected calcium
• Corrected calcium (mg/dL) = measured total calcium (mg/dL) + [0.8 × (4.0 − albumin)]
•Corrected calcium (mmol/L) = measured total calcium (mmol/L)+ [0.02 × (Normal albumin [40 g/l] – patients albumin)]
E. Renal equations
1.Measured creatinine clearance (CCr) L/day
•[24-h urine creatinine (mg/dL) × 24-h urine volume (L/day)]/serum creatinine (mg/dL)
•CCr ml/min = [(CCr L/day × 1000 ml/L)]/1440 min/day
•CCr ml/min × 1.73/BSA = CCr ml/min/1.73 sq.m
–Normal values = 95 ± 20 mL/min per 1.73 m2 in women and 120 ± 25 mL/ min per 1.73 m2 in men

Appendices |
849 |
|
|
2. Estimated creatinine clearance (CockroftÐGault equation)
• (140 - Age in years × Weight in kg) / Serum creatinine in mg/dl × 72
• For female patient multiply with 0.85
3.Fractional excretion of sodium (FENa+)
[UrineNa+ ] ´[plasma creatinine]
[Urine creatinine] ´[plasmaNa+ ]
–Normal value = <1
4.Fractional excretion of urea (FEurea)
[Urineurea] ´[plasma creatinine]
[BUN] ´[urinecreatinine]
– <35 in prerenal azotemia, 50–65 in acute tubular necrosis
F.Nutrition equations
1.Ideal or predicted body weight (IBW)
• Male IBW (kg) = 50 + (0.91 × (height in cm − 152.4))
• Male IBW (kg) = 50 kg for 5 ft; add 2.3 kg for every 1 in. above 5 ft
•Female IBW (kg) = 45.5 + (0.91 × (height in cm − 152.4))
•Female IBW (kg) = 45.5 kg for 5 ft; add 2.3 kg for every 1 in. above 5 ft
2.HarrisÐBenedict equation with LongÕs modiÞcation (calories requirement)
• For women, basal metabolic rate (BMR) = 65.5 + (9.6 × weight in kg) + (1.8 × height in cm) − (4.7 × age in years)
•For men, BMR = 66 + (13.7 × weight in kg) + (5 × height in cm) − (6.8 × age in years)
•Actual energy needs=BMR×AF×IF (AF, activity factor; IF, injury factor)
•Activity factor (AF): Confined to bed = 1.2; out of bed = 1.3
• Injury factor (IF): Minor surgery = 1.2; skeletal trauma = 1.3; major sepsis = 1.6; severe burn = 2.1
•Normal calories requirement = 25–30 kcal/kg of predicted body weight
3.Protein requirement
•1 g of nitrogen = 6.25 g of protein
•Non-protein calories (NPC)–nitrogen ratio = 150:1
•Nitrogen balance = (protein intake/6.25) − (24-h urinary urea nitrogen + 4)
•Negative nitrogen balance >5 = severe stress
• 1 g of nitrogen loss = 30 g lean body mass lost
•1 g of glucose = 4 kcal
•1 g of protein = 4 kcal
•1 g of lipid = 9 kcal
•Protein loss in dialysis = 4–6 g/h in hemodialysis; 40–60 g in peritoneal dialysis
4.Respiratory quotient (RQ):
•Carbon dioxide production (VCO2)/oxygen consumption (VO2)
•Normal value on balanced diet = 0.7–1.0
•> 1: Excess carbohydrate
•<0.7: Excess fat

850 |
Appendices |
|
|
G.Intra-abdominal pressure equation
•Abdominal perfusion pressure (APP) = mean arterial pressure (MAP) − IAP (intra-abdominal pressure)
•Normal intra-abdominal pressure = 5–7 mmHg
•Filtration gradient (FG) = glomerular filtration pressure (GFP) − proximal tubular pressure (PTP) = MAP − 2 × IAP
H.Statistical equations
•Sensitivity: True positives/(true positive [TP] + false negative [FN])
•Specificity: True negative/(true negative [TN] + false positive [FP])
•Positive predictive value: True positive/ (true positive + false positive)
•Negative predictive value: True negative/(true negative + false negative)
•Positive likelihood ratio (LR+): sensitivity/(1 − specificity)
•Negative likelihood ratio (LR−): (1 − sensitivity)/specificity
•Prevalence (pretest probability): (TP + FN)/(TP + FP + TN + FN)
•Pretest odds: Prevalence/(1 − prevalence)
•Posttest odds: Pretest odds × LR
•Posttest probability: Posttest odds/(posttest odds + 1)
•Event rate (ER): Total events/total subjects (event + nonevent)
•Absolute risk reduction (ARR): Control event rate (CER) − experimental event rate (EER)
•Relative risk reduction (RRR): (CER − EER)/CER
•Relative risk (RR): EER/CER
•Odds ratio: (experimental event [EE]/experimental nonevent [EN])/(control event [CE]/control nonevent [CN])
•Number needed to treat (NNT): 1/ARR
•Number needed to harm (NNH): 1/(CER − EER)
• |
Rate of Type I error = Number of False positives = Alpha |
• |
Rate of Type II error = Number of False negatives = Beta |
•Power of a test = (1-Beta) I. Neurology equations
•CBF = (CAP − JVP) ÷ CVR
(CBF, cerebral blood flow; CAP, carotid artery pressure; JVP, jugular venous pressure; CVR, cerebrovascular resistance)
•CPP = MAP − ICP
(CPP, cerebral perfusion pressure; MAP, mean arterial pressure; ICP, intracranial pressure)
– Keep CPP between 60 and 75 mmHg
•Increased WBC in traumatic tap:
Rule of thumb: Subtract one WBC for every 500–1,500 RBCs (if peripheral WBC is normal)
J.Hematology equation
•ANC = WBC × [(segs/100) + (bands/100)] (ANC, absolute neutrophil count)
•Corrected reticulocyte count (CRC)= reticulocytes (%) ´ Hct (L / L)
0.45L/L