

- •Contents
- •1. Pharmacokinetics
- •3. Practice Questions
- •2. Antiarrhythmic Drugs
- •3. Antihypertensive Drugs
- •3. Anticonvulsants
- •5. Opioid Analgesics
- •8. Drugs of Abuse
- •1. Antibacterial Agents
- •4. Antiprotozoal Agents
- •1. Histamine and Antihistamines
- •3. Drugs Acting on Serotonergic Systems
- •1. Drugs Used in Diabetes
- •2. Steroid Hormones
- •6. Endocrine Drug List
- •1. Anticancer Drugs
- •1. Immunopharmacology
- •1. Toxicology
- •2. Toxicology Practice Questions
- •Index
Anticancer Drugs |
1 |
PRINCIPLES AND DEFINITIONS
Log-Kill Hypothesis
Cytotoxic actions ofanticancer drugs follow first-orderkinetics: Theykilla fixed percentage oftumor cells, not a fixed number one rationale for drug combi nations.
Growth Fraction
Cytotoxic drugs are more effective against tumors that have a high growth frac tion (large percentage actively dividing). Normal cells with high growth fraction (e.g., bonemarrow) are also more sensitive to anticancer drugs.
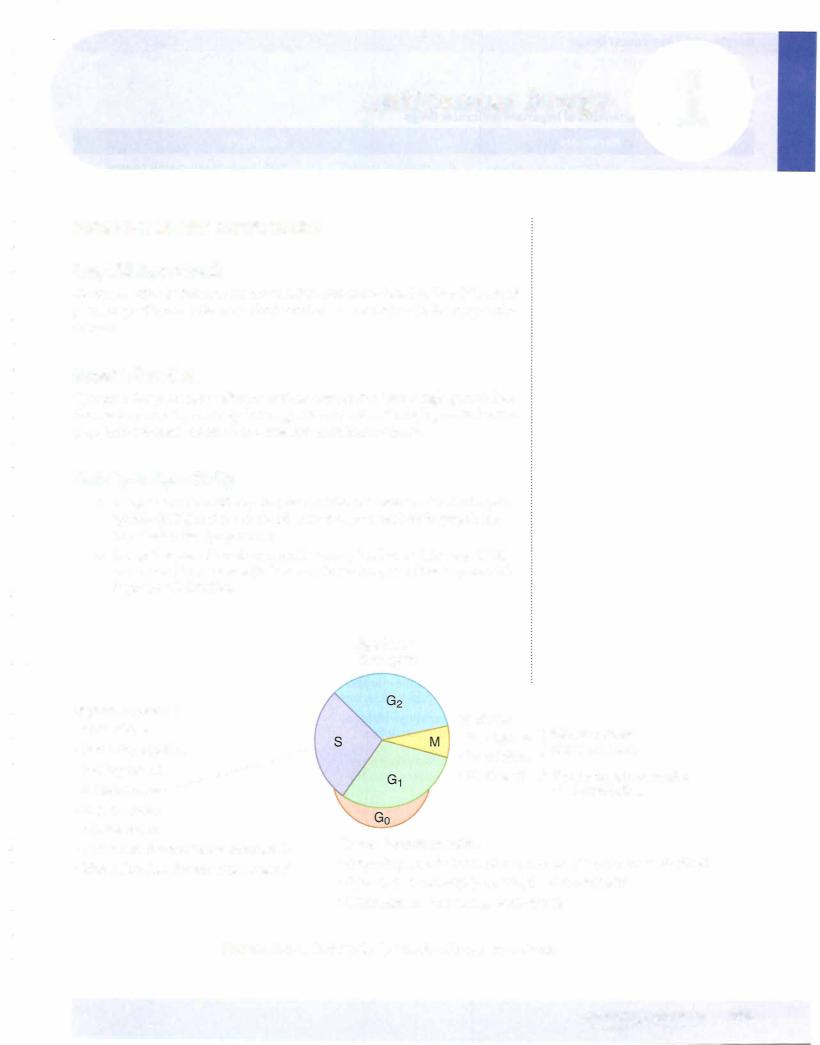
Cell-Cycle Specificity
•Drugs that act specifically on phases ofthe cell cycle are called cell-cycle specific (CCS) and are more effective in tumors with high-growth frac tion (leukemias, lymphomas).
•Drugs that are cell-cycle nonspecific (many bind to and damage DNA) can be used in tumors with low-growth fraction, as well as tumors with high-growth fraction.
G2 phase
Bleomycin
•phase specific
•Cytarabine
•6-mercaptopu ine
•6-thioguanine
•5-fluorouracil
•Methotrexate
•Hydroxyurea
•lrinotecan (blocks topoisomerase I)
Etoposide (blocks topoisomerase II)S
M• phase
• Vinblastine
• V.mens. t"me
Paclitaxel
}Blocks tubular polymerization
}Blocks depolymerization of microtubules
•Non-cell-cycle specific
• Alkylating agents (cyclophosphamide, cisplatin, procarbazine)
• Antitumor antibiotics (doxorubicin, daunorubicin)
Figure IX-1 -1 . Cell-Cycle Specificity of Anticancer Drugs
|
295 |
MEDICAL |

Section IX • Anticancer Drugs
DRUGS
Table IX-1-1. Characteristics of Important Anticancer Drugs
Drug
Cyclophosphamide
Cisplatin
Procarbazine
Doxorubicin
Methotrexate
(CCS)
5-Fluorouracil (CCS)
Capecitabine (oral)
6-Mercaptopurine (CCS)
Bleomycin (CCS)
Mechanism
Alkylating agent-attacks guanine N7-dysfunctional DNA
Alkylating agent- cross-links DNA strands
Alkylating agent
lntercalator, forms free radicals, inhibits topoisomerase
Antimetabolite-inhibits
DHF reductase (S phase)
Pyrimidine antimetabolite (S p hase) bioactivated
to inhibit thymidylate synthetase
Purine antimetabolite (S phase) bioactivated by HGPR transferase
Complexes with Fe and 02DNA strand scission (G2 phase)
Uses
Non-Hodgkin, ovarian, breast cancer, neuroblastoma
Testicular, ovarian, bladder, lung cancer
Hodgkin
Hodgkin, breast, endometrial, lung, and ovarian cancers
Leukemias, lymphomas, breast cancer; rheumatoid arthritis, psoriasis
Breast, ovarian, head, and neck cancer-topical for basal cell cancer and
keratoses; colorectal cancer
Acute lymphocytic leukemia; immunosuppression
Hodgkin, testicular, head, neck, skin cancer
Vinblastine (CCS) |
J, Microtubular |
Vinblastine-Hodgkin, |
|
Vincristine |
polymerization-spindle |
testicular cancer, Kaposi |
|
poisons (M phase) |
Vincristine-Hodgkin, |
||
|
|||
|
|
leukemias, Wilms |
Side Effects
BMS, hemorrhagic cystitis (mesna, traps acrolein and is protective)
Nephrotoxicity (use amifostine); neurotoxicity (deafness)
BMS, leukemogenic
BMS-delayed CHF (dexrazoxane is an iron-chelating agent preventing the formation of free radicals; it is not a free radical "trapper")
BMS, leucovorin (folinic acid) rescue
BM5
BMS
Pneumonitis, pulmonary fibrosis
BMS
Neurotoxicity
All-trans retinoic |
Differentiating agent, |
Acute myelogenous |
"Differentiation syndrome" with |
acid (ATRA) |
promotes differentiation of |
leukemia (AML), M3 |
respiratory distress, pleural and |
|
promyelocytes |
|
pericardiaI effusions, CNS symptoms |
Definition ofabbreviations: BMS, bone marrow suppression; CCS, cell-cycle specific; CHF, congestive heart failure; GI, gastrointestinal.
Clinical Correlate
Thymineless Death of Cells
Flucytosine (FC) and 5-fluorouracil (5-FU) are bioactivated to 5-fluorodeoxyuridine (5-FdUMP), which inhibits thymidylate synthetase "thymineless death" of fungal cells (FC) or neoplastic cells (5-FU).
296 MEDICAL

Chapter 1 • Anticancer Drugs
TOXICITY OF ANTICANCER DRUGS
Table IX-1-2. Other Dose-Limiting or Distinctive Toxicities
Toxicity |
Drug(s) |
Renal |
Cisplatin,* methotrexate |
Pulmonary |
Bleomycin,* busulfan, procarbazine |
Cardiac |
Doxorubicin, daunorubicin |
Neurologic |
Vincristine,* cisplatin |
lmmunosuppressive |
Cyclophosphamide, methotrexate |
Other |
Cyclophosphamide (hemorrhagic cystitis); |
|
procarbazine (leukemia); asparaginase* |
|
(pancreatitis) |
*Less BMS-"marrow sparing"
•Rapidly proliferating cells, such as the bone marrow, gastrointestinal tract mucosa, hair follicles, and gonads are the most sensitive to cyto toxic drugs.
•Most often bone marrow suppression (BMS) is dose limiting.
•Anticancer drug dosage is usually carefully titrated to avoid excessive neutropenia (granulocytes <500/mm3) and thrombocytopenia (platelets <20,000/mm3).
•Colony-stimulating factors, erythropoietin, and thrombopoietin can be supportive ---infections7J, and need for antibiotics (see table below).
Table IX-1-3. Clinical Uses of Cytokines
Cytokine |
Clinical Uses |
Aldesleukin (IL-2) |
i Lymphocyte differentiation and i NKs-use in |
|
renal cell cancer and metastatic melanoma |
lnterleukin-11 |
i Platelet formation-used in thrombocytopenia |
Filgrastim (G-CSF) |
i Granulocytes-used for marrow recovery |
Sargramostim (GM-CSF) |
i Granulocytes and macrophages-used for |
|
marrow recovery |
Erythropoietin |
Anemias, especially associated with renal failure |
Thrombopoietin |
Thrombocytopenia |
MEDICAL 297

Section IX • Anticancer Drugs
RESISTANCE TO ANTICANCER DRUGS
Another rationale for combination drug regimens in cancer is to prevent or delay the emergence ofresistance.
Table IX-1-4. Modes of Resistance to Anticancer Drugs
Mechanism |
Drugs or Drug Groups |
Change in sensitivity (or I level) or .t binding |
Methotrexate, vinca alkaloids, |
affinity of target enzymes or receptors |
estrogen and androgen recep |
Decreased drug accumulation via I expression |
tors |
Methotrexate, alkylating |
|
of glycoprotein transporters, or .t permeability |
agents |
Formation of drug-inactivating enzymes |
Purine and pyrimidine |
|
antimetabolites |
Production of reactive chemicals that "trap" |
Alkylators, bleomycin, |
the anticancer drug |
cisplatin, doxorubicin |
Increased nucleic acid repair mechanisms |
Alkylating agents, cisplatin |
Reduced activation ofprodrugs |
Purine and pyrimidine |
|
antimetabolites |
Chapter Summary
•The "log-kill" hypothesis states that cytotoxic anticancer agents kill a certain percentage, not a fixed number, of cells.
•Cytotoxic drugs are most effective against rapidly dividing cells.
•Drugs that act on proliferating cells are cell-cycle specific and are usually also cycle-phase specific. Figure IX-1-1 illustrates the cell cycle and the drugs acting in each cycle phase.
•Drugs that act on nonproliferating cells are dose-dependent and cell-cycle independent.
•Rationales forcombination drug usage are that each drug will independently kill a fixed percentage and that one drug will still kill a cancer cell that has developed resistance to a different drug in the cocktail.
•Rapidly proliferating normal cells are more sensitive to cytotoxic drugs.
Bone marrow suppression often determines the upper limit oftolerable chemotherapy. Table IX-1-1 lists mechanisms of action, selected clinical uses, and side effects of major anticancer drugs. Table IX-1-2 shows the dose-limiting and distinctive toxicities of anticancer drugs.
•Table IX-1-4 summarizes the modes of resistance developed by cancers toward specific anticancer drugs.
298 MEDICAL

Anticancer Drug |
2 |
|
|
Practice Questions |
|
1 . Which o f the following chemotherapeutic drugs inhibits the polymeriza tion of microtubules but is not associated with causing bone marrow sup pression?
A.
Cyclophosphamide
B.Cisplatin
c.5-Fluorouracil
D.Vinblastine
E.Vincristine
2.A patient with non-Hodgkin lymphoma is to be started on the CHOP regimen, which consists of cyclophosphamide, doxorubicin, vincristine, and prednisone. Which one ofthe following agents is most likely to be protective against the toxicity of doxorubicin?
A.Amifostine
B.Dexrazoxane
c.
D.
Leucovorin
Mesna
E.Vitamin C
3. A drug used in a chemotherapy regimen works by complexing with iron and oxygen to promote DNA strand breaks. While on this drug the patient must be monitored closely due to pulmonary side effects. In what phase of the cell cycle does this drug work?
A.G1
B.S
C.Gz
D.M
E.This drug is not cell-cycle dependent.
4.Resistance to which anticancer drug, used in leukemias, lymphomas, and breast cancer, is associated with increased production of dihydrofolate reductase?
A.Doxorubicin
B.Vinblastine c. 6-MP
D.Cytarabine
E.Methotrexate
MEDICAL 299
Section IX • Anticancer Drugs
5.A patient undergoing cancer chemotherapy has an increase in urinary frequency with much discomfort. No specific findings are apparent on physical examination. Laboratory results include hematuria and mild leu kopenia, but no bacteria or crystalluria. Ifthe symptoms experienced by the patient are drug related, what is the most likely cause?
A. Cyclophosphamide
B.
c.
5-FU
Methotrexate
D.Prednisone
E.Tamoxifen
Answers
1 .
2.
Answer: E. Only two of the drugs listed do not cause bone marrow suppres sion: cisplatin and vincristine. Only two ofthe drugs listed inhibit microtubule plymerization: vinblastine and vincristine. The drug that fits both categories is vincristine. Patients on vincristine should be monitored for neurotoxicity, espe cially peripheral neuropathies.
Answer: B. Dexrazoxane is an iron-chelating agent that prevents the formation of free radicals and reduces the cardiotoxicity ofanthracyclines such as doxorubicin. Amifostine is protective of nephrotoxicity caused by cisplatin. Folinic acid (leu covorin) reduces the toxicity of methotrexate because it provides an active form offolate to normal (nonneoplastic) cells, resulting in "leucovorin rescue." Mesna, which inactivates acrolein, is available for protection against hemorrhagic cystitis in patients treated with cyclophosphamide.
3.Answer: C. It helps to know which anticancer drugs are cell-cycle specific and which have characteristic toxicities. Bleomycin forms a complex with iron and oxygen and promotes DNA strand breaks. Its major side effects are pulmonary toxicities including pneumonitis and fibrosis. It acts acting mainly in the G2 phase ofthe cell-cycle.
4.Answer:E. Methotrexate is a widely-used chemotherapydrug that is also com monly used in moderate to severe rheumatoid arthritis. It inhibits the enzyme dihydrofolate reductase (DHFR) thereby reducing the synthesis of tetrahydro folate and thus inhibiting DNA synthesis. Resistance occurs when cancer cells upregulate DHFR or alter the binding of methotrexate to DHFR.
5.Answer: A. These symptoms are those of a mild case of hemorrhagic cystitis. Bladder irritation with hematuria is a fairly common complaint of patients treated with cyclophosphamide. It appears to be due to acrolein, a product formed when cyclophosphamide is bioactivated byliver P450 to form cytotoxic metabolites. Mesna is the antidote used to detoxify acrolein and protect against hemorrhagic cystitis.
300 MEDICAL

SECTION
lmmunopharmacology
