

Атлас по рентгенологии травмированных собак и кошек / an-atlas-of-radiology-of-the-traumatized-dog-and-cat
.pdf82 Radiology of Thoracic Trauma
Case 2.35
2

Lung injury 83
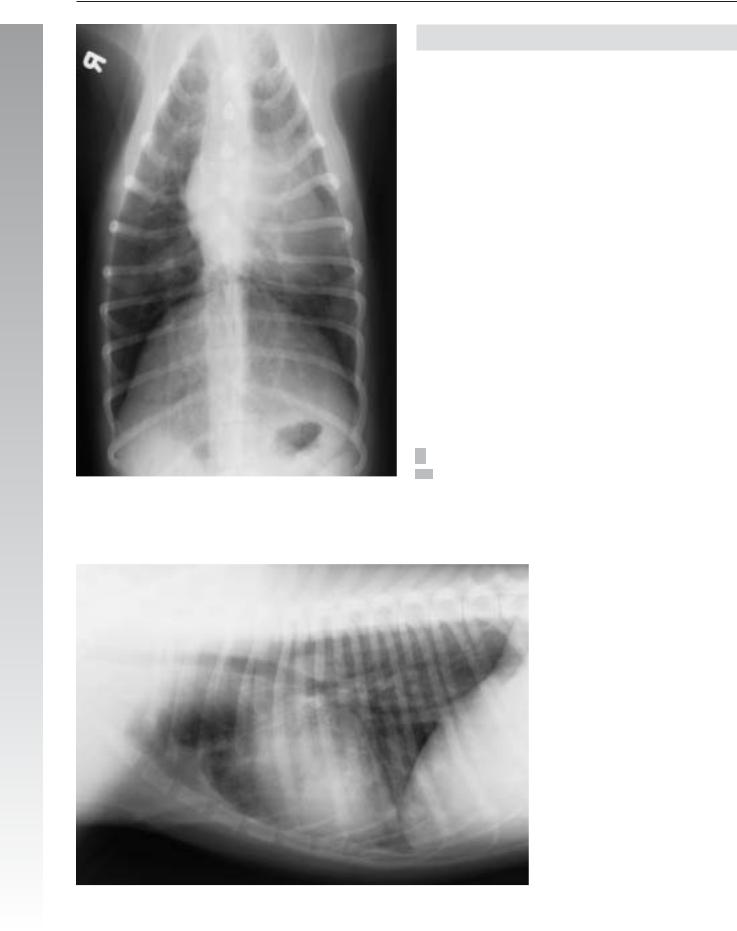
Signalment/History: “Kila” was an 18-month-old, female Golden Retriever who had been hit by a car 24 hours earlier.
Physical examination: She could not walk when presented for treatment. However, she had a superficial pain reflex, a normal panniculus reflex, and normal patellar reflexes.
Radiographic procedure: Studies were made of the thorax because she was a trauma case. Additional views were made centering on the thoracic spine.
Radiographic diagnosis: An accumulation of alveolar fluid in the right lobes caused alveolar patterns. No air-bron-
chograms could be identified clearly. No pleural fluid was noted. The diaphragm was intact. The chest wall was normal. The cranial mediastinum was thought to be widened, especially considering the rather thin body wall.
A fracture-luxation of T5– 6 was noted (arrow).
2
Treatment/Management: Because the presence of pain perception is a favorable finding, “Kila’s” fracture was treated. Treatment was in the form of a body cast with the dog positioned beneath a metal “grate” to prevent movement. Later radiographs made after clinical recovery showed the affected vertebra to have remained in position.
84 Radiology of Thoracic Trauma
Case 2.36
Signalment/History: “Harvey”, an 8-month-old, male Hound, had a history of having been found recumbent by the side of the road. The owners admitted that he had not been
2 well recently and had been coughing. The case was registered as a possible “hit by a car”.
Radiographic procedure: Radiographs of the thorax were made because of the clinical history of a young dog with a cough.
Radiographic diagnosis (day 1): A disseminated diffuse increase in pulmonary density involved both the interstitium and peribronchiolar tissues. In addition, a poorly marginated, 5-cm-in-diameter mass was located distally in the right middle lobe. Interstitial nodularity was adjacent to the mass lesion. A round, well-marginated, 2-cm mass lay dorsal to the tracheal bifurcation and was possibly a mediastinal lymph node. A slight separation of the pulmonary lobes suggested pleural fluid. The diaphragm was located caudally and flattened. The apex of the cardiac silhouette was shifted to the left chest wall, possibly as an effect of pleural adhesions. Focal pleural thickening was evident on the left chest wall also suggesting chronic pleural disease.
Day 1
Lung injury 85
Radiographic diagnosis (10 months following the surgical removal of the right cranial and middle lobes due to foreign body induced bronchopneumonia): The marked tracheal deviation to the right, right-shift of the cardiac silhouette, and herniation of the left cranial lung apex into the right hemithorax were all postsurgical. The pleural thick-
ening and fluid collection in the cranial portion of the right 2 hemithorax were the effects of the chronic pleuritis plus pos-
sible postsurgical changes. Generalized peribronchial thickening suggested persistent chronic bronchial disease, while the prominent air bronchograms ventrally suggested a more recent pneumonia.
Treatment/Management: “Harvey” was quickly seen on the first study to have chronic lung disease with a possible mass lesion. Following unsuccessful medical treatment, he was treated surgically with removal of the pneumonic lung lobes that were secondary to a foreign body.
Comments: The frequency of inhalation of plant awns with associated pulmonary infection is influenced by the geographical location and is dependent on the presence of wild grasses and a dry climate. “Harvey” was typical of many of these patients in that he continued to suffer from pulmonary disease as seen on the follow-up radiographs. The role of possible trauma from being struck by a car was not important in this patient.
10 months later

86 Radiology of Thoracic Trauma
2.2.5Pulmonary hematoma
Case 2.37
2

|
Pulmonary hematoma |
87 |
|
Signalment/History: “Corky” was a 5-year-old, male |
for a period this long after trauma suggested a secondary pneu- |
||
Golden Retriever who had been struck by a car 10 days pre- |
monia following the original pulmonary hemorrhage. The left |
||
viously and had been hospitalized since that time. He was re- |
hemidiaphragm was caudal and flattened. Minimal pleural flu- |
||
ferred to this clinic for the repair of his pelvic fractures. |
id, probably the result of hemorrhage, was trapped around the |
||
|
injured left lung. The dorsal crus of the diaphragm on the right |
||
Physical examination: On physical examination, he was |
could not be identified due to silhouetting with the pneu- |
||
8–10 % dehydrated, febrile, and had harsh lung sounds espe- |
monic lobe. The retrosternal lymph node was enlarged. |
2 |
|
cially on the left. |
Treatment/Management: “Corky” had a cardiac arrest and |
||
|
|||
Radiographic procedure: Radiographs were made of the |
died 48 hours after the radiographic study. |
|
|
thorax for the first time since the trauma. |
At necropsy, a hematoma was identified on the cranial aspect |
||
|
|||
Radiographic diagnosis (day 10 post trauma): Massive |
of the left caudal lung lobe. Lung sections from the right cau- |
||
thoracic wall injury was seen with fractures of 5 ribs on the left |
dal lobe had hemorrhage, fibrinous exudate, and parenchymal |
||
with a marked displacement of the fragments. Unequal filling |
necrosis typical of an acute coliform pneumonia. It was sus- |
||
of the left lung fields was evident. Caudal lobe hyperinflation |
pected that E. coli had been present at the time of the injury as |
||
with generalized increased peribronchial shadows was present. |
a bacteremia and had subsequently localized in the injured |
||
A sharply defined soft tissue mass, 2 x 3 x 3 cm in size, situat- |
caudal lobes, which provided a good culture medium. The |
||
ed possibly in the caudal aspect of the left cranial lung lobe was |
distribution of the necrosis was different to the cranioventral |
||
probably a post-traumatic hematoma (arrows). This was in- |
distribution typical of aerogenous pneumonias. The pleural |
||
dicative of a severe lung injury with parenchymal damage, |
fluid had become infectious in nature. Myocardial injury was |
||
which had permitted the pooling of blood within the pul- |
present, but was limited to the outermost one-fifth of the |
||
monary parenchyma. |
myocardium. The retrosternal lymph node was not examined. |
||
An infiltrative pattern in the right caudal lobe included an airbronchogram. The presence of this type of infiltrative pattern

88 Radiology of Thoracic Trauma
Case 2.38
2
Signalment/History: “Kami” was a 4-year-old, male Lhaso
Apso who had been bitten by a large dog.
Physical examination: The examination was difficult because of the size of the dog and because of the severe dyspnea.
Radiographic diagnosis: Both views of the thorax were attempted, although it was thought that the positioning would not be good.
Radiographic diagnosis: The large volume of generalized subcutaneous air compromised the evaluation of the intrathoracic injury. The injury to the intercostal muscles was bilateral and resulted in an increase in the distance between the injured ribs. Most severe was the fracture of the 5th rib on the right, with fragment displacement. The pulmonary injury affected the right middle lobe, which showed an increase in fluid density due to hemorrhage. However, a more prominent injury on the right was in the caudal lobe (arrows) and caused a wedge-shaped pulmonary lesion indicative of an obstructive atelectasis or possibly a large pulmonary hematoma. The diaphragm was intact. Free pleural air was pocketed on the right. The sternal changes were congenital.
Treatment/Management: Despite the bilateral injury to the thoracic wall and the obstructive atelectasis, “Kami” recovered nicely with conservative treatment.

Interstitial nodules 89
2.2.6Interstitial nodules
Case 2.39
2
Day 1
Signalment/History: “Little Girl”, a 9-month-old, female DSH cat, had a history of dyspnea characterized by rapid breathing. She had been listless for several months. Fecal examination was negative for lungworms.
Radiographic procedure (day 1): A patchy infiltrative pattern was present throughout the lungs with a tendency toward nodular formation. No pleural fluid could be seen. The diaphragm was intact but caudal in position. The cardiac silhouette was normal in size, shape, and position. The differential diagnosis included any granulomatous lesion. A metastatic tumor was not considered because of the age of the patient.
Treatment/Management: The cat was treated with antibiotics without any improvement in her medical status.

90 Radiology of Thoracic Trauma
2
Day 25
Radiographic diagnosis (day 25): Further coalescence of the pulmonary nodules was seen with patches of emphysematous lung. Minimal pleural fluid was present. A granulomatous pneumonia remained the most likely diagnosis.
Treatment/Management: Because of the poor prognosis associated with the lack of improvement in the status of the kitten, the owners chose to have the patient euthanized. Necropsy examination showed a marked involvement of all lung lobes. Pus could be forced from the lung upon application of pressure. The nodules were generally between 1 and 2 cm in diameter. The alveoli were distended and contained a cellular population of macrophages and PMN cells. The macrophages were filled with fat indicative of a chronic, lipid inhalation pneumonia. The alveolar walls were thickened.
Presented with this information, the owner said that she had been giving the cat oil daily to prevent “hair balls”. Without a history of chronic administration of oil, a definitive diagnosis could not have been reached from the radiographs and physical examination alone.

Diaphragmatic hernia 91
2.2.7Diaphragmatic hernia
Case 2.40
2
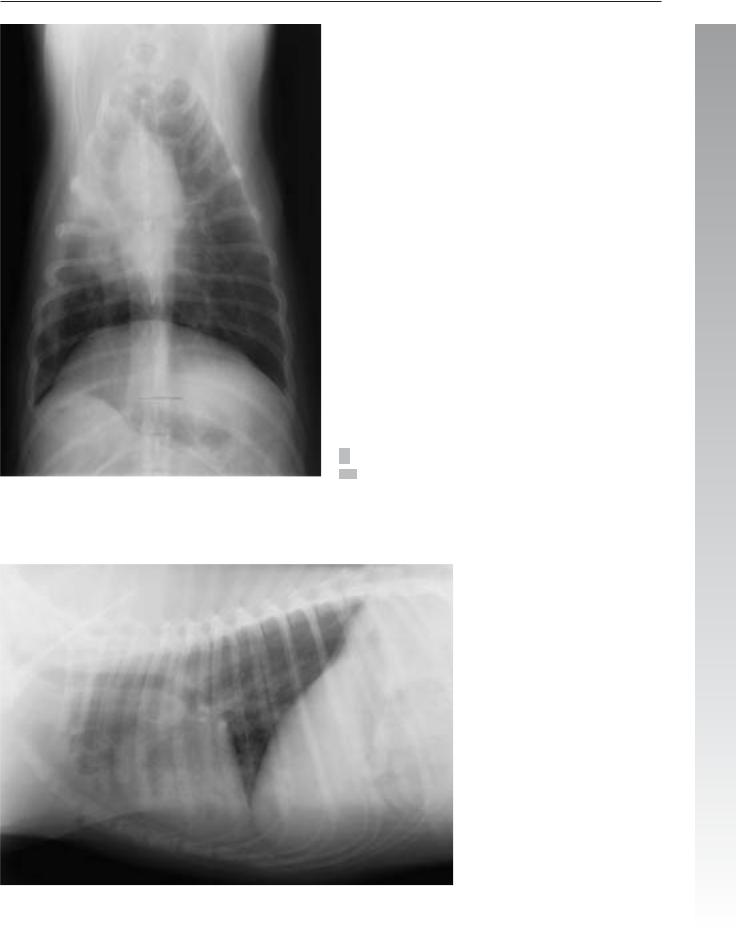
Signalment/History: “Sir” was a 6-month-old, male Miniature Poodle, who had been struck by a car 12 hours earlier.
Physical examination: No heart or lung sounds could be detected on the right side.
Radiographic procedure: The thorax was radiographed.
Radiographic diagnosis: The right hemithorax was filled with air-filled loops of small bowel. The heart was displaced to the left and elevated. The diaphragm could not be seen on either view. The increase in fluid density within the thoracic cavity was due to a contusion of the lungs, pleural fluid, and the fluid density of the bowel. The airand ingesta-filled stomach was identified in a near-normal location in the abdomen. The 4th rib on the right was fractured near the costovertebral joint.
Treatment/Management: The diagnosis was rather easy because the air-filled loops of bowel lay within the thoracic cavity. The owners decided to have the hernia repaired at another clinic and took the poodle home.