

Атлас по рентгенологии травмированных собак и кошек / an-atlas-of-radiology-of-the-traumatized-dog-and-cat
.pdf52 Radiology of Thoracic Trauma
2.2.3Pleural fluid
Case 2.17
2
Signalment/History: This mature, female DSH cat was a stray that was found by the new owner to have a prominent swelling on the right side of her body.
Physical examination: The prominent soft tissue mass was easily palpable and the contents could be readily compressed.
Radiographic procedure: Whole body radiographs were made.
Radiographic diagnosis: The soft tissue swelling was centered around the last ribs on the right and contained discretely outlined air-filled structures thought to be bowel loops. The stomach was enlarged and fluid-filled suggesting the possibility of a pyloric obstruction. No injury to the chest wall was seen except for injury to the last asternal ribs on the right. The diaphragm was intact. The lungs appeared normal. No pleural fluid was noted.
Treatment/Management: The owner refused treatment of the paracostal hernia and the cat was lost to follow-up. The bowel loops were not distended and the possibility of a bowel obstruction was considered minimal; still, the owners were advised that surgical repair was recommended.
Pleural fluid 53
Case 2.18
2
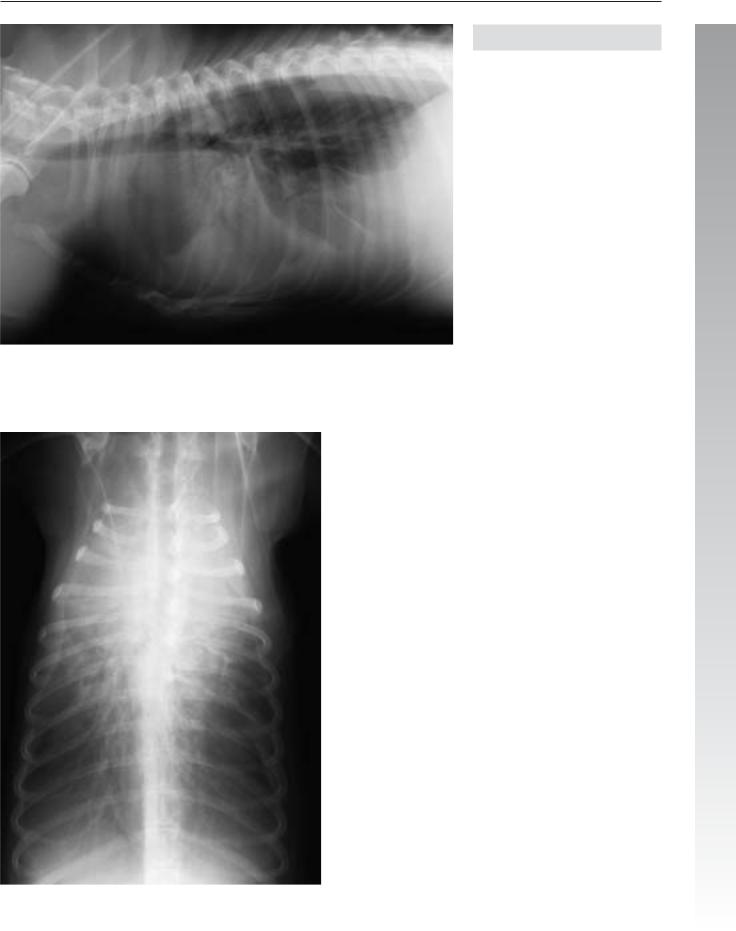
Signalment/History: “Olive” was a 2-year-old, female Old English Sheepdog with a history of being unable to breathe when placed in dorsal recumbency. She became acutely dyspneic when positioned on her back and the owners believed she had been shot by the neighbors.
Radiographic procedure: Studies of the thorax were ordered because of the history of dyspnea.
Radiographic diagnosis: A massive pleural effusion was present, characterized by retraction of the lung lobe margins from the thoracic wall. The cardiac silhouette was difficult to evaluate, but was probably normal in size, shape, and position. The lung fields were also difficult to evaluate, but the cranial main-stem bronchi were folded caudally suggesting the presence of a cranial intrathoracic mass. The diaphragmatic shadows were difficult to assess, but they appeared to be located caudally and were flattened. No evidence of chest wall injury was noted. A severe congenital sternal anomaly resulted in only 5 or 6 segments being present.
Treatment/Management: Treatment was medical and the possibility of lung lobe torsion was not proven.

54 Radiology of Thoracic Trauma
Case 2.19
Signalment/History: “August” was a 4-month-old, male Australian Shepherd who had been in a dogfight two days pre-
viously.
2
Physical examination: An injury to the left thoracic wall could be palpated. It was possible to insert several fingers between the displaced ribs.
Radiographic procedure: Radiographs were made of the thorax.
Radiographic diagnosis (day 1): Disruption of the caudal ribs on the left was associated with intercostal muscle tearing, soft tissue swelling in the thoracic wall, and minimal subcutaneous emphysema; all of which were indicative of a massive puncture wound. Extensive pleural bleeding in the left hemithorax and collapse of the underlying lung lobes resulted in a mediastinal shift to the right. Note the cavitary lesion in the left caudal lobe that represents a traumatic pneumatocele. The tracheal shadow was elevated as a result of the heart moving into the right hemithorax. The presence of hemorrhage within the mediastinum could not be evaluated.
Day 1

Pleural fluid 55
2
Day 2
Radiographic diagnosis (day 2, DV view only): Radiographs done the next day showed a lesser amount of pleural fluid with an increase in the aeration of the left lung lobes.
Day 4
Radiographic diagnosis (day 4, DV view only): Radiographs taken two days later showed a worsening of the condition with a marked increase in the amount of pleural fluid causing a more extensive mediastinal shift to the right. Note the shifting of the carina (arrow). The left lung did not appear
to contain any air at this time.

|
56 Radiology of Thoracic Trauma |
|
Treatment/Management: Surgery to remove the hemor- |
|
rhaging left caudal lung lobe was performed on day 4. Radio- |
|
graphs made on day 10 showed a partial aeration of the re- |
|
maining lung lobes on the left. The left hemidiaphragm was |
|
shifted cranially and the accessory lobe had shifted into the left |
2 |
hemithorax. All of these changes resulted in a minimal medi- |
astinal shift to the left. The rib injuries were not treated. |
Detection of a traumatic pneumatocele indicated a more severe injury to the lung than expected with a typical blunt trauma, and suggested that lobectomy might be required to stop the hemorrhage.
The possibility of abdominal organ injury was considered because of the caudal location of the injury; however, treatment for an abdominal injury was not required.
Day 10

|
|
Pleural fluid 57 |
|
|
|
|
of atelectasis. Mediastinal widening was suspected to be the |
|
|
Case 2.20 |
|
|
||
|
result of a hemomediastinum with the possibility of organized |
|
||
|
|
|
||
|
|
blood clots within that structure. This was more evident on |
|
|
Signalment/History: “Duke” was a 7-year-old, male Ger- |
the VD view. |
|
||
man Shepherd with a history of having sustaining stab wounds |
A diffuse pulmonary pattern was noted throughout the lungs |
|
||
to the thorax three days earlier. He had been given emergency |
2 |
|||
treatment and was referred with a history of hemothorax that |
without evidence of an air-bronchogram pattern. The cardiac |
|||
had been increasing in volume as shown by daily thoracic ra- |
silhouette was identified and thought to be within normal lim- |
|
||
diographs. |
its; however, the examination was compromised by the pres- |
|
||
|
|
ence of pleural fluid. The failure to identify a displacement of |
|
|
Physical examination: He was thought to be in DIC at the |
the lung lobes or mediastinum suggested an absence of any |
|
||
time of admission to the hospital and was having PVCs. |
pleural masses. The minimal soft tissue thickening noted on |
|
||
|
|
the left thoracic wall was assumed to be secondary to the trau- |
|
|
Radiographic procedure: The thoracic study included both |
ma. |
|
||
VD and DV views. |
No evidence of peritoneal fluid was noted. Minimal spondy- |
|
||
|
|
|
||
Radiographic diagnosis: The pleural fluid was massive and |
losis deformans was evident in the caudal thoracic spine. |
|
||
was freely movable when the DV and VD views were com- |
Small circular shadows on the lateral view are attachments for |
|
||
pared. It was suspected to be hemorrhage because of the his- |
|
|||
tory. The fluid pooled around the right middle lobe and the |
the leads from the EKG machine. |
|
||
caudal portion of the left cranial lobe, indicating some degree |
|
|
|
|

58 Radiology of Thoracic Trauma
2
Day 1

Pleural fluid 59
2
Day 25
Radiographic diagnosis (day 25): Resolution of the pleural fluid was remarkable along with the identification of normal pulmonary bronchovascular markings.
Treatment/Management: Stab wounds are a different form of trauma from the more common blunt chest trauma resulting from automobile accidents. The absence of alveolar fluid and the presence of pleural fluid instead suggested a puncturetype wound to the lungs. An important aspect in this case could be seen on comparison of the DV and VD views of the first study that showed not only the amount of pleural fluid and how freely it moved, but the relatively uninjured lung lobes as well. The diaphragm was not visualized on the DV view but was thought to be normal on the VD projection.
If the injury was truly a “stab wound” resulting in pleural and mediastinal hemorrhage, why was not a pneumothorax present as well? A thoracic wall injury secondary to a stab wound probably closes immediately and does not permit air to enter the thoracic cavity. In this case, it seems possible that the lung lobes had not been injured and the bleeding had resulted from some other vascular injury.
The presence of secondary pneumonia is always difficult to determine in trauma cases with lung lobe contusion and/or atelectasis. That was not a problem in this dog. “Duke” recovered completely following conservative treatment and returned to work on the police force.

60 Radiology of Thoracic Trauma
Case 2.21
2
Day 1
Signalment/History: “Roy” was a 4-year-old, male English Pointer with a history of chronic dyspnea. Small quantities of purulent pleural fluid had been aspirated in the past. A grass awn had been removed from the thoracic wall 1 year previously.
Physical examination: Lung sounds could not be auscultated and the heart sounds were muffled. The patient was dyspneic and slow to move.
Radiographic procedure: Thoracic radiographs were made.
Radiographic diagnosis (day 1): Massive pleural fluid was seen on both views and prevented evaluation of the lung lobes. Pleural fluid had infiltrated into the fissures between the lung lobes. The bronchi and pulmonary vessels could not be seen completely, but they were thought to be in their normal position, which ruled out any pulmonary mass lesions. The diaphragm could not be completely identified ventrally. The thorax was widely expanded.

Pleural fluid 61
2
Day 2
Radiographic procedure (day 2): Radiographs were made on day 2 following the removal of 675 ml of purulent pleural fluid. The lung lobes could be better evaluated A fluid-dense mass was noted within the accessory lobe, which silhouetted with the heart shadow and the diaphragm. A minimal pneumothorax probably secondary to the placement of the needle for aspiration of the pleural fluid was present. The normal position of the gastric air bubble helped to rule out a diaphragmatic hernia.
Treatment/Management: Chronic trauma was considered in this patient, but the nature of the pleural fluid was strongly suggestive of an inflammatory lesion. The geographical location in which the dog lived had grass awns. This fact, plus the past history of grass awn migration into the thoracic wall, suggested that abscessation within the accessory lobe was the primary diagnosis. The dog was operated and the affected lobe removed. A grass awn was identified as the cause of the abscess. Recovery of the patient was difficult because of the chronic infection.