

Essentials of Orthopedic Surgery, third edition / 01-Basic Science of Bone and Cartilage Metabolism
.pdf1. Basic Science of Bone and Cartilage Metabolism |
31 |
FIGURE 1-28. Radiograph of humerus of patient with history of deep-sea diving. The sclerotic area represents infarction of the marrow cavity with formation of calcium soaps and new bone from the reparative margins. (From Bogumill GP. Orthopaedic Pathology: A Synopsis with Clinical Radiographic Correlation. Philadelphia: Saunders, 1984. Reprinted by permission.)
segment develops a reactive hyperemia and resorbs. The necrotic bone then appears to be more dense on the radiograph—so-called relative radiodensity. There is also some compaction of dead trabeculae; as well as marrow necrosis with subsequent saponification and calcification of the dead fat, to additionally explain the sclerotic changes seen on radiographs.
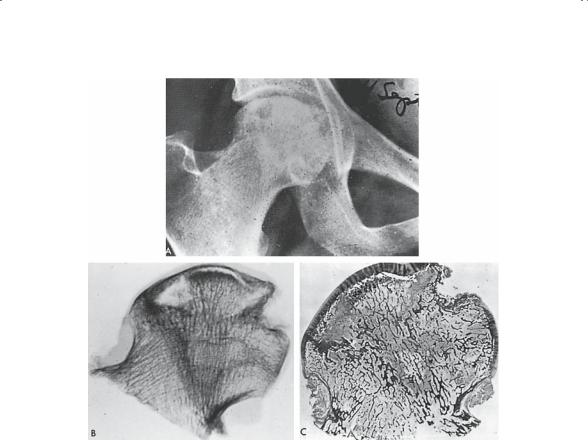
A number of vasoocclusive phenomena can cause avascular (aseptic) necrosis (AVN). Although AVN can involve any number of different sites, the femoral head is by far the most typical (Fig. 1-29).
Etiologies of AVN can be grouped by causation:
1.Trauma: damage to vessels supplying the segment of the bone in question (i.e., fractures of the femoral neck and scaphoid).
2.Occlusive phenomena:
32 J.N. Delahay
FIGURE 1-29. Clinical radiograph (A), specimen radiograph (B), and corresponding macrospecimen (C) of femoral head from a 26-year-old patient on long-term steroid therapy for idiopathic thrombocytopenic purpura with progressive pain and disability of both hips. Note the crescent sign, a cleft beneath the articular cartilage resulting from compression fractures of dead trabeculae. Also note the lytic areas in the lateral aspect of the femoral head caused by revascularization with removal of dead trabeculae and replacement with viable fibrous tissue. Zones of increased density are also evident. (From Bogumill GP. Orthopaedic Pathology: A Synopsis with Clinical Radiographic Correlation. Philadelphia: Saunders, 1984. Reprinted by permission.)
a.Emboli: such as fat in alcoholism and pancreatitis; nitrogen as in Caisson’s disease
b.Stasis: coagulopathies and hemaglobinopathies
c.External constriction: vasculitis such as systemic lupus erythematosus (SLE) and inflammatory bowel disease
d.External compression: typical of storage diseases (Gaucher’s and Fabry’s) where stored material compresses intraosseous arterioles
3.Idiopathic: the causative factor is unknown, as in steroid-induced osteonecrosis and Chandler’s disease.
1. Basic Science of Bone and Cartilage Metabolism |
33 |
Hematologic Syndromes
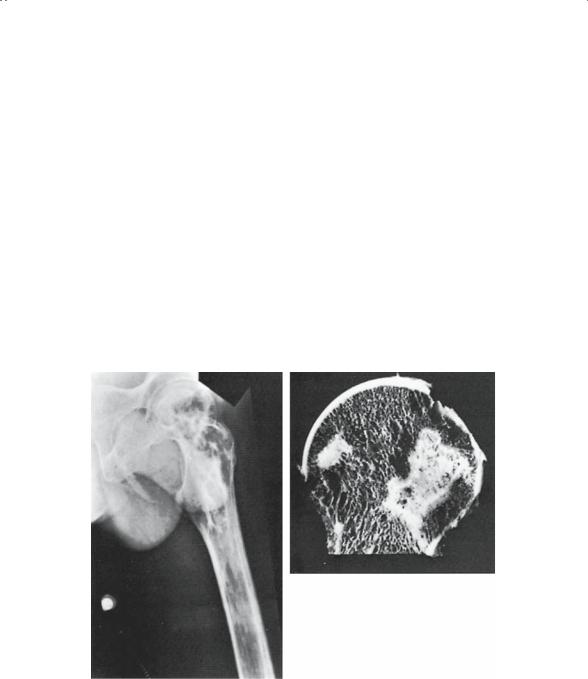
The genetic hemoglobinopathies, although not truly circulatory diseases, are best remembered in this group. Sickle cell disease, and to a lesser degree thalassemia, produce skeletal changes primarily through two mechanisms: myeloid hyperplasia and vasoocclusive phenomena. Because of the anemia these patients suffer, there is a drive to increase medullary hematopoiesis, and this results in dilation of bony contours to accommodate a marrow driven to produce more blood. Widening of the diploe of the skull, dilation of the small bones of the hands and feet, and increased trabecular markings are all radiographic hallmarks of this process. The vasoocclusive effect of these distorted red cells causes bone infarcts similar to those previously discussed (Fig. 1-30).
However, in a select group of patients the infarcts are frequently painful and a component of the “painful crisis.” The stasis, sludging, and dead bone create a comfortable environment for bacterial invasion, accounting for the increased incidence of osteomyelitis in these patients.
B
A
FIGURE 1-30. (A) Radiograph of hip and proximal femur of a 25-year-old man with sickle cell anemia. Areas of mottling and sclerosis are seen, suggestive of bone infarction. Evidence of sequestrum formation is seen in the lateral femoral cortex (bone within a bone). (B) Gross specimen of the femoral head taken from the same patient. Light necrotic areas are well demarcated from viable bone. (From Johanson NA. Musculoskeletal problems in hemoglobinopathy. Orthop Clin North Am 1990;21(1):196. Reprinted by permission.)

34 J.N. Delahay
Neurodevelopmental Disorders
The final diagnostic category discussed in this chapter is the most heterogeneous of all. There are a few common threads that can be found to tie this eclectic mix of clinical states together. Clearly, they all have an impact on the musculoskeletal system. An attempt is made to describe them generically and use an example in each category to underscore their impact on the skeleton.
Neurologic Diseases
The deficit produced by neurologic diseases can be either sensory, motor, or central in origin. The level of involvement will determine the skeletal changes. Central nervous system deficits are typified by cerebral palsy. Prenatal anoxia can cause damage to the cerebral cortex; this includes damage to neural tissue that normally inhibits or damps muscular tone and keeps it at an acceptable level. Without normal inhibitory influences, these muscles become spastic. Muscle spasticity existing over a protracted period results in muscle imbalance around joints. Ultimately, contractures and chronic joint deformities such as subluxations and dislocations will follow. The hip, for example, is of particular concern in the spastic child.
Poliomyelitis is an example of a motor deficit disease. Viral damage to anterior horn cells results in focal motor weakness in various muscle groups in the extremities. Bone deprived of normal muscle loading tends to become osteopenic. In addition, the variable nature of the involvement again causes muscle imbalance around joints, with its subsequent deformities.
Sensory deficits may result in neuropathic arthritis. Joints deprived of proprioception are rapidly destroyed. The aggressive sequence of microtrauma, repeated effusions, ligamentous incompetence, articular damage, and severe degenerative joint disease is the fate of patients with tertiary lues, diabetes, pernicious anemia, leprosy, and heavy metal intoxications. Although proprioception is the initial sensory component lost, pain fiber deficit usually follows, resulting in destroyed but painless joints.
Spina bifida, or myelodysplasia, may result in mixed deficits. This congenital defect combines motor and sensory deficits to produce skeletal changes that parallel both. Osteopenia, joint deformity, and joint destruction may all be found. The joints, as expected, are insensate, a fact that only compounds the clinical problems.
Developmental/Congenital Defects
It is important to remember that congenital defects (present at birth) need not be genetic, and vice versa. However, any process that impacts on the growing skeleton, whether it be congenital or developmental, can be expected to produce changes. These changes can generally be expected to

1. Basic Science of Bone and Cartilage Metabolism |
35 |
be alterations in the configuration of the bone itself. Shortening, bowing, or angular deformities may be seen. Changes in bone density may or may not be seen.
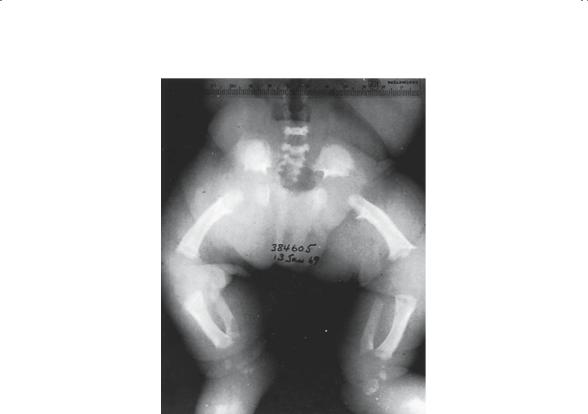
Achondroplasia is the most common dwarfing syndrome. It follows an autosomal dominant inheritance pattern (Fig. 1-31). This syndrome disrupts normal enchondral bone growth and, therefore, results in shortening of all bones that depend on this mechanism for their growth (Fig. 1-32).
A B
FIGURE 1-31. (A) Posterior photograph of achondroplastic dwarf showing distorted growth of long bones. The proximal limb segments are proportionately shorter than the distal, with the hands reaching only to the hip region. The legs are bowed, and the scapulae and pelvis are smaller than normal. Scoliosis is uncommon. (B) Lateral photograph of child with achondroplasia. Note marked lumbar lordosis with prominent buttocks as a result of pelvic tilt. The lordosis is caused in part by differential growth of vertebral body versus posterior elements. (From Bogumill GP. Orthopaedic Pathology: A Synopsis with Clinical Radiographic Correlation. Philadelphia: Saunders, 1984. Reprinted by permission.)
36 J.N. Delahay
FIGURE 1-32. Radiographic appearance of lower limbs in a patient with achondroplasia. Note the narrow sciatic notch and flat broad acetabulum resulting from inadequate growth of “Y” cartilage in acetabulum. Shortened, thick femurs, fibias, and fibulas are bowed. Bone density is normal. Epiphyses do not yet exhibit secondary ossification centers. (From Bogumill GP. Orthopaedic Pathology: A Synopsis with Clinical Radiographic Correlation. Philadelphia: Saunders, 1984. Reprinted by permission.)
Bone dysplasias (intrinsic defects of bone growth) are, as a general rule, genetic in origin despite the fact that some of the milder (tarda) forms may not be apparent until the child begins growing.
Chromosomal defects, such as Down syndrome, are often characterized by severe ligamentous laxity. This is the basis for the numerous orthopedic conditions that are typical in this group. Atlantoaxial instability, flat feet, patellar subluxation, bunions, and subluxation of the hips all point to the inability of the ligamentous structure to stabilize joints. Many of the chromosomal abnormalities involve defects in mesoderm development, which accounts for the common coincidence of musculoskeletal, genitourinary, and cardiac abnormalities.
The clubfoot deformity is probably multifactorial in its etiology. The interplay of heredity and environment is accepted, although poorly understood. Clubfoot, similar to developmental dysplasia of the hip and scolio-

1. Basic Science of Bone and Cartilage Metabolism |
37 |
sis, is a defect that is considered to be a reflection of this interplay. Usually identified at birth, clubfoot is a generalized dysplasia of the mesenchymal structures (bone, ligament, muscle) of the foot and perhaps the entire lower extremity. Genetic as well as environmental (intrauterine position) factors have been implicated, but their exact interaction remains unknown.
Summary
Many different pathologic states have impact on the skeletal system, whether they be primary or secondary. Bone has a limited number of ways of responding to abnormal stimuli whether they be chemical, mechanical, infectious, or circulatory. In general, one can expect to see either bone resorption or bone formation, either locally or systemically, dominate the pattern. A working knowledge of the normal mechanism usually allows the observer to anticipate the response to many of these pathologic processes.
In this regard, observing the changes that one sees on standard imaging studies often permits the development of a working differential diagnosis. Using the basic seven disease categories and expanding each into a plausible list of diagnoses should lead, given more data, to a definitive diagnosis and hence appropriate treatment.
Suggested Readings
Bernstein J. Musculoskeletal Medicine. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2003.
Bogumill GP. Orthopaedic Pathology: A Synopsis with Clinical and Radiographic Correlation. Philadelphia: Saunders, 1984.
Buckwalter JA. Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2000.
Questions
Note: Answers are provided at the end of the book before the index.
1-1. Osteoporosis results in:
a.Increase in skeletal mass
b.Decrease in the amount of mineralized bone
c.No change in the mineral to matrix ratio
d.Decrease in the cortical diameter of a long bone
e.Increase in bone mineral density by DEXA scanning

38 J.N. Delahay
1-2. Paget’s disease of bone is:
a.A disease of decreased bone turnover
b.Common in young males
c.Rarely seen in the skull
d.Is most common in the foot
e.None of the above
1-3. Bone as a tissue:
a.Is largely devoid of cells
b.Contains more water than cartilage
c.Contains type II collagen in its ground substance
d.Depends on its lamellar structure for strength
e.Has amorphous calcium phosphate as its major mineral constituent
1-4. Neurologic diseases such as cerebral palsy, polio, and spina bifida damage the musculoskeletal system. This damage is primarily the result of:
a.Muscle imbalance
b.Lack of sensation
c.Recurrent infections
d.Defects in sensory motor integration
e.Mental retardation
1-5. Causes of rickets include all except:
a.Sprue
b.Genetic renal tubular defects
c.Vitamin C deprivation
d.Dilantin therapy
e.Renal phosphate retention 1-6. Hyaline cartilage:
a.Is a hypocellular tissue
b.Depends on the glycosaminoglycans for resiliency
c.Is primarily water by weight
d.Is found in diarthrodial joints
e.All the above
1-7. Achondroplasia:
a.Is an aberration of epiphyseal growth
b.Is the most common skeletal dysplasia
c.Is characterized by knock knees
d.Is often associated with mental retardation
e.Is fatal in infancy
1-8. Rheumatoid arthritis:
a.Is a disease of the articular cartilage
b.Typically results in hyperostosis around the joints
c.Commonly causes early fibrosis of the synovium
d.Is considered a noninflammatory arthritis
e.Radiographically is characterized by juxtaarticular osteopenia

1. Basic Science of Bone and Cartilage Metabolism |
39 |
1-9. All the following are characterized by generalized osteopenia on the radiograph except:
a.Gout
b.Hyperparathyroidism
c.Osteomalacia
d.Multiple myeloma
e.Osteoporosis
1-10. Neuropathic arthritis is the result of proprioceptive sensory loss in conjunction with microtrauma and a component of vasomotor instability. All the following can cause a neuropathic arthritis except:
a.Syphilis
b.Polio
c.Diabetes
d.Heavy metal intoxication
e.Leprosy
1-11. Avascular necrosis of bone:
a.Can result from exogenous steroid administration
b.Is characterized by relative radiodensity
c.Can involve the femoral head and talus among other bones
d.Can be associated with sickle cell disease
e.All the above
1-12. Collagen:
a.Is a proteoglycan
b.Is important for the compressive strength of cartilage
c.Is synthesized by chondroblasts and osteoblasts
d.Is a large ring molecule
e.Is not a cross-linked molecule