

Essentials of Orthopedic Surgery, third edition / 06-Sports Medicine
.pdf6. Sports Medicine |
267 |
Symptoms that occur with activity and improve with rest are typical of overuse injuries. Nocturnal awakening usually indicates more serious injury or an underlying systemic disorder. Such a distinction is important in distinguishing shin splints from a stress fracture in a long-distance runner. Are there any specific activities that might cause symptoms? In the athlete with intermittent knee symptoms, pain in the anterior aspect of the knee that is worse with stair climbing or with prolonged sitting suggests problems related to the patellofemoral joint. Symptoms that occur predictably with cutting and pivoting activities, accompanied by swelling and instability, suggest an internal derangement of the knee such as a meniscus injury or tear of the anterior cruciate ligament.
Physical Examination
The specific examination depends on the nature of the symptoms and the region affected. Each anatomic region and orthopedic condition have pertinent special tests. All physical examinations, however, should begin with inspection and observation of the extremity. After acute injury one should compare the injured joint in question to its opposite side. Inspection for skin changes such as ecchymoses, abrasions, and associated swelling can be important clues in distinguishing macrotrauma from a microtraumatic event. Range of motion of the joint in question both actively and passively is imperative. First have the athlete move the joint in question and observe for associated pain or asymmetry as compared to the opposite side. Examples include a patient who presents with shoulder pain of insidious onset whose active and passive range of motion is asymmetrical and limited on the affected side suggesting an adhesive capsulitis as a diagnosis; this is compared to a rotator cuff injury where passive range of motion would be full despite a limited active range of motion secondary to pain. Other examples would be the active inability to extend one’s knee after acute injury despite nearly full passive range of motion, suggesting injury (rupture) of the extensor mechanism that could be seen in patellar tendon or quadriceps tendon ruptures.
Strength assessment is an important component to the exam of any jointrelated injury. During strength assessment, weakness may be the result of direct injury to a musculotendinous unit responsible for joint function. However, pain, guarding, or reflex inhibition of muscular contraction can also be responsible for perceived weakness on examination. The ability of the sports medicine professional to examine the athlete in the acute setting shortly after the injury (before pain and swelling set in) is especially helpful in obtaining an accurate assessment of strength. Although relatively uncommon, injuries to nerve and vasculature structures can and do occur and should be ruled out as a precipitating cause of injury, especially in the acute setting. Their examination is an essential component of a complete physical examination.
268 J.J. Klimkiewicz
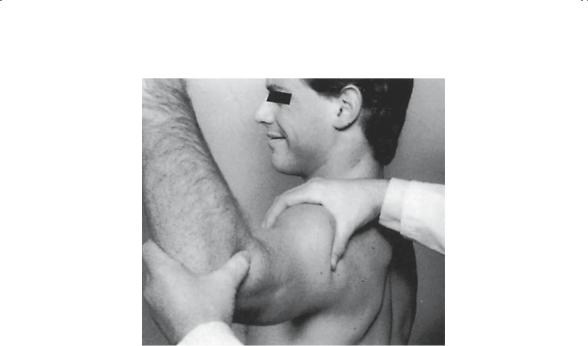
FIGURE 6-5. Examining for anterior instability, the apprehension test is performed by placing the shoulder in a provocative position of abduction and external rotation. Gentle anterior pressure is placed on the humeral head in this position, seeking to elicit patient apprehension as an indication of shoulder instability. (From Hawkins RJ, Bokor DJ. Clinical evaluation of shoulder problems. In: Rockwood CA, Matsen FA (eds) The Shoulder, vol. 1. Philadelphia: Saunders, 1990:149–177. Reprinted by permission.)
On initial examination one should always keep an open mind for referred symptoms. In addition to examining the joint in question, one should also focus particularly on the adjacent joints, as well as the spine, for a contributing role in the symptoms. Examples include a slipped capital femoral epiphysis (SCFE) of the hip in an adolescent with knee pain, or a cervical disk herniation as a cause for shoulder discomfort.
Applying special examination techniques specific to the area in question and suspected diagnosis completes the physical examination. These techniques can be found in their respective chapters. Examples of special tests include impingement signs in case of shoulder pain, or apprehension in the case of shoulder instability as the arm is placed in a position of abduction and external rotation (Fig. 6-5).
Special Tests
X-Rays
Radiographs are mandatory in any athlete with a history of trauma where macrotraumatic injury is in question. Microtraumatic injuries do not usually

6. Sports Medicine |
269 |
demonstrate radiographic findings when a soft tissue component is suspected as a cause for pain. One exception, however, is when an osseous component is thought to be a cause for pain in the absence of trauma (i.e., stress fracture). In this setting, X-rays are helpful as an initial screening tool. When negative, other special tests such as magnetic resonance imaging (MRI) or bone scintigraphy can be especially helpful.
Specifically obtained stress views can be useful in assessing joint integrity. Common examples include stress views taken for grade III sprains of the acromioclavicular joint (Fig. 6-6).
Magnetic Resonance Imaging
Revolutionizing our ability to visualize soft tissues and establish diagnoses noninvasively, MRI is an exceptional diagnostic tool. In addition to
FIGURE 6-6. (A) Note the slight deformity at the acromioclavicular (AC) joint of this patient’s left shoulder, sustained from landing directly on the point of the shoulder. (B) Note that with the application of weights to the patient’s wrists, the slight deformity is exaggerated, and the AC joint displacement is easily seen; this is known as a stress view of a “separated shoulder.” (From Rockwood CA, Green DP (eds) Fractures, 2nd ed, vol 3. Philadelphia: Lippincott, 1984. Reprinted by permission.)

270 J.J. Klimkiewicz
demonstrating precise anatomic detail, MRI gives us a precise physiologic window with which to see various inflammatory, metabolic, and traumatic conditions. It is helpful in diagnosing both microtraumatic as well as macrotraumatic injuries. Variation in software techniques allows precise imaging of osseous structures, tendons, ligaments, menisci, and articular cartilage. The addition of intraarticular contrast has been especially helpful in the shoulder and hip in the diagnosis of injuries to the labral structures. MRI has emerged as the most common imaging modality within the field of sports medicine. It should be used judiciously, however, secondary to cost and not overshadow a thorough history and physical examination.
Bone Scintigraphy
Bone scans generate images based on dynamic physiology rather than static structure. Increased tracer uptake can occur because of a number of conditions and is pathognomonic for any one particular injury. Interpretation should be carried out in the context of history, physical examination, and routine X-rays. For example, in a runner with progressively increasing leg pain in which a bone scan displays focal uptake in the midtibia, a stress fracture is likely (Fig. 6-7).
FIGURE 6-7. Bone scan of the tibia in a runner with leg pain reveals focal uptake at the junction of the midand distal third tibia, consistent with a stress fracture. (From DeLee JC, Drez Jr D (eds) Orthopaedic Sports Medicine: Principles and Practice, vol 2. Philadelphia: Saunders, 1994. Reprinted by permission.)

6. Sports Medicine |
271 |
Arthroscopy
Most commonly applied to the knee, shoulder, ankle, elbow, and hip, arthroscopy is the gold standard for definitive diagnosis and treatment of joint-related injuries. Its utility in diagnosis is especially helpful in situations where all other diagnostic testing has been unsuccessful in establishing a diagnosis. Its overwhelming use in the field of sports medicine, however, is predicated on the treatment of joint injuries once a diagnosis is reached; for more-complex problems it often serves as an invaluable diagnostic tool.
Treatment of Sports Injuries
Treatment of macrotraumatic and microtraumatic injuries follows an algorithmic approach. The goals of treatment are to reduce pain, inflammation, swelling, and stiffness initially followed by an increase in strength and function to allow expeditious return to normal function and athletic activity. Treatment can be divided into three distinct but overlapping phases: immediate, early, and definitive.
Macrotraumatic Injuries
Immediate
Immediate treatment begins at the time of injury and involves the pneumonic “RICE” (rest, ice, compression, and elevation). Immobilization of the joint in the early stages after an injury with these treatment principles act to limit the initial swelling. By accomplishing this purpose, local soft tissue edema and pain are minimized; this often allows the treating physician an accurate physical exam, leading to a good working diagnosis, and the need for definitive tests can also be determined.
Early
Early treatment involves establishing a definitive diagnosis and minimizing the sequelae of trauma including joint stiffness and muscle atrophy. Often additional testing is required in this stage to help formulate both the diagnosis and the definitive treatment plan.
Late
Most macrotraumatic sports injuries are successfully treated nonoperatively, with physical rehabilitation necessary to provide normal strength and motion. Specific indications for operative management vary with the injury in question and its outcomes with different treatment options, as well as the athlete’s goals and expectations both on and off the athletic

272 J.J. Klimkiewicz
field. Surgical intervention may involve traditional open techniques or, more commonly, an arthroscopic approach to limit the morbidity imposed by a surgical approach.
Microtraumic Injuries
Immediate
Rest, in the treatment of overuse injury, does not necessarily require crutches, cast, or sling, but it does mean activity modification. Any activity that causes the athlete’s symptoms should be avoided. The tissues involved must be allowed to rest to heal and resolve the inflammatory process causing their symptoms. For athletes, this aim often requires restriction from their sport.
Early
During the period of activity modification, a number of techniques can be helpful to further relieve pain and inflammation to restore normal function; these can begin with the use of nonsteroidal antiinflammatory drugs (NSAIDs). Various modalities such as ice, heat, electrical stimulation, ultrasound, and massage can all be of some help in decreasing pain and associated swelling.
Late
Although activity modification is the mainstay of treatment, with a prolonged period of inactivity muscular atrophy as well as overall deconditioning can result. Definitive treatment for these injuries often involves a dedicated physical therapy program aimed at restoring the athlete’s strength and endurance required for a return to sport. Focus on the athlete’s biomechanics is also an essential component in treating overuse injuries to prevent their recurrence. Attention to specifics of the supporting structures is often helpful in this regard. Alignment problems are often identified in this phase of treatment for lower extremity injuries. Fabrication of a shoe lift orthotic for a previously unrecognized leg-length discrepancy or a medial longitudinal arch support for overpronation can lead to a more-successful return to activity. Sometimes videotape analysis of the activity or technique is helpful to identify, correct, and prevent poor mechanics.
Occasionally, overuse injuries do not respond to nonoperative measures and surgical correction is required. Conditions occasionally associated with failure of conservative treatment include lateral epicondylitis, shoulder impingement, and patellar/Achilles tendonitis. Failure of conservative treatment in these cases involves long courses (often 6 months to 1 year)

6. Sports Medicine |
273 |
of conservative management. Rarely, stress fractures are in high-risk areas (i.e., hip) or fail to respond to adequate immobilization and require surgical intervention.
Summary and Conclusion
As the numbers of active individuals continue to grow, so does the field of sports medicine. Emphasis at present within this field focuses on the prevention of injuries as well as minimizing the effects of surgery through less-invasive approaches such as arthroscopy. As knowledge within this field continues to grow, accomplishing the goal of a successful return to sport both safely and expeditiously becomes feasible. Appreciation of the basic science as it relates to these injuries and the means in which they are treated is essential in bridging the gap between the practice of clinical medicine and the successful return to the athletic field.
Suggested Readings
DeLee JC, Drez D Jr, Miller MD (eds) Orthopaedic Sports Medicine: Principles and Practice, 2nd ed. Philadelphia: Saunders, 2001.
Garrick JG, Webb DR. Sports Injuries: Diagnosis and Management. Philadelphia: Saunders, 1990.
Griffin LY (ed) Orthopaedic Knowledge Update: Sports Medicine. American Academy Orthopaedic Surgeons. Philadelphia: Saunders, 1994.
McGinty JB (ed) Operative arthroscopy, 2nd ed. Philadelphia: Lippincott-Raven, 1996.
Questions
6-1. Which best describes a tendon’s histologic makeup and biomechanical function?
a.Primarily made up of fibroblasts to effectively resist tensile forces
b.Primarily made up of fibroblasts to resist compressive forces
c.Primarily made of type I collagen to resist compressive forces
d.Primarily made of type I collagen to resist tensile forces
e.Primarily made of proteoglycan to resist tensile forces
6-2. A ballet dancer presents with a 6-month history of pain surrounding the ankle without any particular injury. Tenderness is present along the posteromedial aspect of her ankle. Which structure is most commonly associated with this overuse injury?
a.Achilles tendon
b.Peroneal longus

274J.J. Klimkiewicz
c.Peroneal brevis
d.Flexor hallicus longus
e.Extensor digitorum longus
6-3. Which best describes a grade III ligamentous injury?
a.Macroscopic injury associated with microscopic damage resulting in stretching of a ligament. Partial compromise in ligamentous strength.
b.Microscopic injury with no macroscopic injury. No functional compromise of strength.
c.Complete macroscopic ligamentous rupture with partial structural integrity remaining.
d.Complete macroscopic ligamentous rupture without any structural integrity remaining.
e.None of the above.
6-4. Muscle strains are most commonly caused by:
a.Concentric muscle contraction
b.Eccentric muscle contraction
c.Direct traumatic force
d.Laceration
e.None of the above
6-5. Articular cartilage is biomechanically most effective in resisting:
a.Compression
b.Tension
c.Rotation
d.Shear
e.Corrosion
6-6. Which type of meniscal tear has the best potential for healing?
a.Horizontal tear
b.Radial tear
c.White–white tear
d.White–red tear
e.Red–red tear
6-7. Which best describes a microtraumatic injury pattern?
a.Anterior shoulder dislocation
b.Lateral ankle sprain
c.Stress fracture of hip
d.Patellar dislocation
e.None of the above
6-8. Initial management of Achilles tendonitis includes:
a.Nonsteroidal medication
b.Activity modification
c.Physical therapy
d.Corticosteroid injection
e.Surgical debridement

6. Sports Medicine |
275 |
6-9. Histologically, ligaments attach to bone via which microscopic entity?
a.Proteoglycan
b.Fasciles
c.Type V collagen
d.Sharpey’s fibers
e.Myofibroblasts
6-10. The primary unit of tendon structure is:
a.Fascicle
b.Endotenon
c.Epitenon
d.Paratenon
e.Musculotendinous unit