

346 |
A n t i b i o t i c E s s e n t i a l s |
If positive, this indicates chronic HBV; if negative, then low-level immunity or false-positive anti-HBV core remain as possible explanations; since distinguishing between these possibilities cannot be done, we recommend immunization with the hepatitis B vaccine series.. It is useful to measure HBV serologic markers periodically in this population, as improvement in immune status due to ART may lead to increasing titers of HBSAb and subsequently confirm immunity..
Therapeutic Considerations: The optimal treatment for HBV infection is in evolution.. Current guidelines suggest treatment of HBV in all patients with active HBV replication, defined as a detectable HBEAg or HBV DNA.. Pending long-term studies defining optimal management, the recommendations set forth in the grid above are reasonable.. Patients being treated with regimens for HBV should be monitored for ALT every 3–4 months.. HBV DNA levels provide a good marker for efficacy of therapy and should be added to regular laboratory monitoring.. The goal of therapy is to reduce HBV DNA to as low a level as possible, preferably below the limits of detection.. The duration of HBV therapy is not well established; with development of HBEAb, while some individuals without HIV can stop therapy after reversion of HBEAg to negative, there are no clear stopping rules for HIV-coinfected patients..
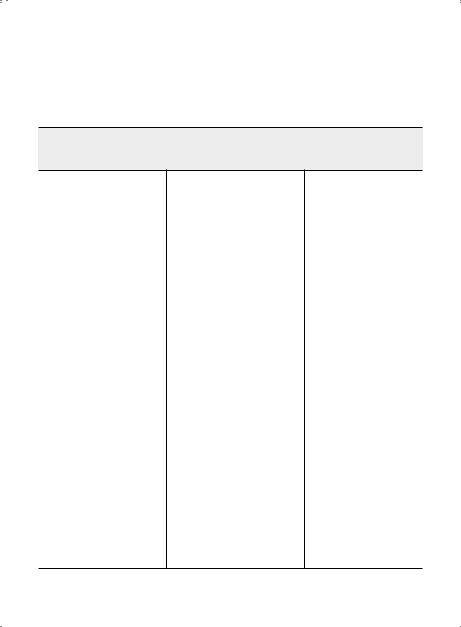
Hepatitis C Virus (HCV)
Subset Pathogens Therapy
HIV Genotype 1 (includes 1a & 1b)
Preferred therapies:
Ledipasvir6 90 mg/sofosbuvir 400 mg (Harvoni) (PO) q24h x 12 weeks
Paritaprevir 150 mg/ritonavir 100 mg/ombitasvir 25 mg (PO) q24h +
dasabuvir7 250 mg (Viekira Pak) (PO) q12h + ribavirin1,2 x weeks3
Sofosbuvir 400 mg (Savaidi) (PO) q24h + Simeprevir4,8 150 mg (Olysio)
(PO) q24h ± ribavirin1 x weeks3
Genotype 2
Preferred therapy:
Sofosbuvir 400 mg (Savaidi) (PO) q24h + ribavirin1 x 12 weeks (16 weeks in cirrhosis)
Genotype 3
Preferred therapies:
Sofosbuvir 400 mg (Savaidi) (PO) q24h + ribavirin1 x 24 weeks Alternate therapy:
Sofosbuvir 400 mg (Savaidi) (PO) q24h + pegylated IFN alfa-2a/2b5
ribavirin1 x 12 weeks
Genotype 4
Preferred therapies:
Ledipasvir6 90 mg/sofosbuvir 400 mg (Harvoni) (PO) q24h x 12 weeks
Paritaprevir 150 mg/ritonavir 100 mg/ombitasvir 25 mg (Viekira Pak
minus dasabuvir) (PO) q24h + ribavirin1 x 12 weeks
Sofosbuvir 400 mg (Sovaidi) (PO) q24h + ribavirin1 x 24 weeks Alternative therapies:
Sofosbuvir 400 mg (Sovaidi) (PO) q24h + pegylated IFN alfa-2a/2b5 +
ribavirin1 x 12 weeks
Sofosbuvir 400 mg (Sovaidi) (PO) q24h + simeprevir8 150 mg (Olysio)
(PO) q24h ± ribavirin1 x 12 weeks
348 |
A n t i b i o t i c E s s e n t i a l s |
Epidemiology: Hepatitis C virus (HCV) infection is transmitted primarily through blood exposure; sexual and perinatal transmission are also possible but less efficient.. A notable exception is sexually transmitted HCV among gay men.. Since modes of transmission of HIV and HCV are similar, there are high rates of HCV coinfection in HIV—an estimated 16% of HIV patients overall, including 80% or more of IDUs and 5–10% of gay men.. Genotype 1 accounts for 75% of HCV in the United States.. HIV accelerates the progression of chronic HCV infection to cirrhosis, liver failure, and hepatocellular carcinoma.. Data are conflicting regarding the independent effect of HCV on HIV disease progression, but several studies have shown a markedly higher rate of antiretroviral therapy-induced hepatotoxicity in those with chronic HCV.. In some series, liver failure from HCV is one of the leading causes of death in HIV/HCV coinfected individuals..
Clinical Presentation: Persistently elevated liver transaminases; usually asymptomatic.. Diagnostic Considerations: All HIV-positive patients should be tested for HCV antibody.. If the antibody
test is negative but the likelihood of HCV infection is high (IDU, unexplained increase in LFTs), obtain an HCV RNA since false-negative antibody tests may occur, especially in advanced HIV disease.. Since LFT elevation does not correlate well with underlying HCV activity, a liver biopsy is the best way to assess the degree of fibrosis and inflammation..
Therapeutic Considerations:
Once Diagnosis is Established.. Advise patients to abstain from alcohol and administer vaccinations for hepatitis A and B (if non-immune).. Also obtain HCV RNA levels with genotype assessment.. HCV RNA levels do not have prognostic significance for underlying degree of liver disease, but higher levels make treatment for cure less likely.. Genotype results also correlate with cure rates (reported cure rates: 60–75% for genotypes 2 and 3; 15–25% for genotype 1).. Some clinicians elect to treat HCV without a liver biopsy due to: the risks, costs, and discomfort of the test; the potential to underestimate the degree of HCV activity due to sampling error; and the high rate of treatment success for genotypes 2 and 3..
Optimal Patient Characteristics for HCV Treatment in HIV include no active psychiatric disease or substance abuse; stable HIV disease with undetectable HIV RNA and higher CD4 cell count; receiving an antiretroviral regimen that does not contain ddl (in particular), d4T, or ZDV; and adherent to medications, follow-up visits, and blood test monitoring.. Only a small proportion of patients will meet all these criteria; therefore, to maximize treatment effect, it is important to optimize clinical status prior to starting HCV therapy.. Patients should be fully educated regarding the goals and risks of treatment, with provision of written information about side effects, local support groups, and whom to contact with questions.. It is useful to administer the first dose of treatment in the office in order to provide instructions on injection techniques..
Choice of Drug Therapy.. The treatment of choice for HCV infection is pegylated interferon plus ribavirin.. All patients should also receive hepatitis A vaccine and counseling to avoid alcohol use..
• Pegylated Interferon. . Two different formulations of pegylated interferon are available for treatment of HCV infection: (1) peginterferon alfa-2a (Pegasys), supplied as a pre-mixed solution and administered subcutaneously as a fixed dose of 180 mcg once a week; and (2) peginterferon alfa-2b (Peg-Intron), supplied as a powder that is reconstituted in saline and administered subcutaneously as a weight-based dose once a week. . Efficacy and toxicity of these two peginterferon preparations appear to be similar.. Three clinical trials have shown that pegylated interferon plus ribavirin is more effective than standard interferon plus ribavirin (N Engl J Med 2004;351:451–9; N Engl J Med 2004;351:438–50; JAMA 2004;292:2839–48).. Interferon has numerous side effects, the most important of which are listed in Table 5..9..
• Ribavirin.. Ribavirin is available in 200-mg capsules.. Although the dose used in clinical trials was 800 mg daily (400 mg BID), it appears that a higher initial dose is associated with greater efficacy.. Standard dose is now 400 mg qAM and 600 mg qPM for weight < 75 kg, and 600 mg qAM and
Chapter 5. HIV Infection |
349 |
600 mg qPM for weight > 75 kg.. Ribavirin causes hemolytic anemia that predictably leads to a measurable decline in hemoglobin; this stabilizes by week 4–8 of treatment.. Hemolytic anemia may be exacerbated in patients receiving ZDV; if possible an alternative NRTI should be chosen, with preference for tenofovir or abacavir. . For symptomatic anemia or patients with coexisting conditions exacerbated by anemia, erythropoietin is used to maintain hemoglobin levels > 10 gm/ dL or higher as needed.. The typical starting dose of erythropoietin is 40,000 units SQ once a week.. ddl is contraindicated during ribavirin administration due to an increased risk of mitochondrial toxicity and hepatic decompensation (Clin Infect Dis 2004;38:e79–e80).. d4T should also be avoided because of its potential for inducing mitochondrial toxicity itself.. Finally, some data suggest that ABC may interact with ribavirin, reducing efficacy of HCV therapy.. Another common side effect of ribavirin is GI distress, which can overlap with a similar effect of interferon.. Ribavirin is pregnancy category × (potent teratogen), and can only be used in sexually active women of childbearing potential if they are using 2 forms of birth control.. Pregnancy should be avoided until at least 6 months after stopping ribavirin..
Monitoring. The monitoring plan for HIV/HCV coinfected patients consists of both safety and efficacy evaluations (Table 5..10).. Results of HCV RNA testing are used to decide between completing 48 weeks of HCV therapy vs.. discontinuing treatment at 12 or 24 weeks due to low probability of cure (Figure 5..3)..
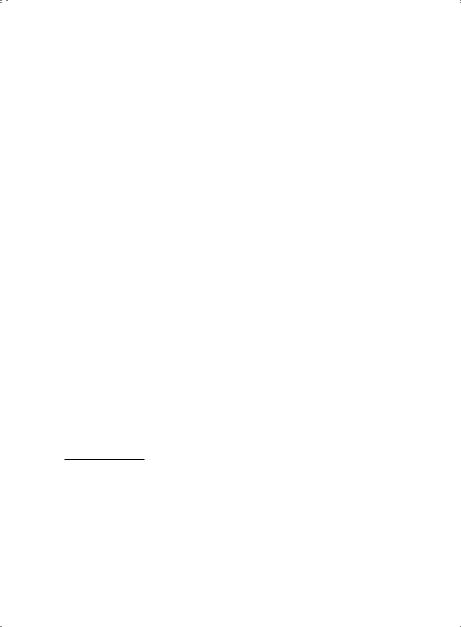
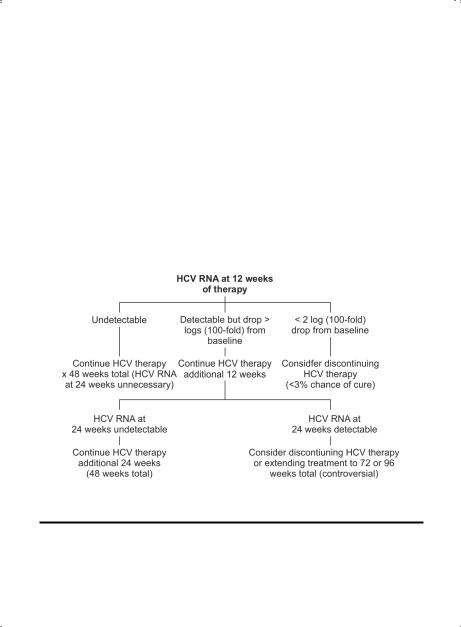
Figure 5.3. Management of HCV Infection Based on HCV RNA Testing
HCV RNA should be assessed at week 12.. If the HCV viral load has not dropped by more than 2 logs (100–fold), then the likelihood of achieving a cure is extremely low.. Many patients and providers will elect to discontinue therapy at this point, although theoretically low-dose peg-interferon may help improve liver fibrosis independent of its antiviral effect.. (This strategy is being tested in clinical trials..) HCV RNA should be measured at weeks 24 and 48.. If undetectable at week 48, additional measurements should be obtained at weeks 4, 12, and 24 after stopping treatment.. An undetectable HCV RNA at week 24 post-treatment is the current standard for assessing a “sustained virologic response” (SVR), which can be equated with cure.. Importantly, patients cured of HCV are susceptible to re-acquisition and should be cautioned about resuming high-risk behavior..

350 |
|
A n t i b i o t i c |
E s s e n t i a l s |
|
|
|
||||||||
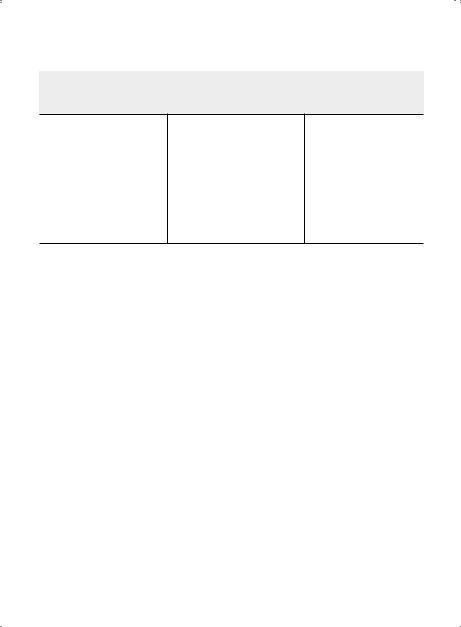
Table 5.9. Adverse Effects Associated with Interferon |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Side Effect |
|
|
|
|
|
|
Comments |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|||||
Fatigue and flu-like |
Dose at night so that some initial symptoms can be slept through.. Symptoms |
|||||||||||||
symptoms (fever, |
may not peak until 48–78 hours after weekly dose and can be managed with |
|||||||||||||
chills, muscle aches, |
acetaminophen (maximum 1300 mg/day) or ibuprofen plus good hydration.. |
|||||||||||||
headache) |
Fatigue is sometimes a manifestation of thyroid dysregulation or anemia; |
|||||||||||||
|
monitor thyroid function tests and CBC |
|
|
|
|
|
||||||||
Depression |
Interferon can aggravate life-threatening psychiatric conditions.. Low threshold |
|||||||||||||
|
for initiating anti-depressant therapy.. Patients with a pre-existing history of |
|||||||||||||
|
depression or other psychiatric disease should be followed closely by mental |
|||||||||||||
|
health professionals during HCV treatment |
|
|
|
|
|
||||||||
Leukopenia, |
Cytopenias are more common in HIV/HCV co-infection.. Can treat with G-CSF |
|||||||||||||
thrombocytopenia, |
300 mcg 3x/week if absolute neutrophil count is < 500/mm3.. If neutropenia |
|||||||||||||
anemia |
persists, decrease dose of interferon.. If platelet count falls to < 80,000/mm3, |
|||||||||||||
|
also consider decreasing interferon dose (some clinicians tolerate counts down |
|||||||||||||
|
to 50,000/mm3).. Low threshold for use of erythropoietin (EPO) 40,000 U/week |
|||||||||||||
|
for anemia (see section on ribavirin) |
|
|
|
|
|
||||||||
Mouth ulcers |
Topical viscous lidocaine or sucralfate is helpful in some |
|
|
|||||||||||
Gastrointestinal |
Nausea and anorexia are the most common, often leading to weight loss.. |
|||||||||||||
symptoms |
Advise patients to eat several small meals daily rather than a few large meals |
|||||||||||||
Hair loss |
Reversible after completion of therapy |
|
|
|
|
|
||||||||
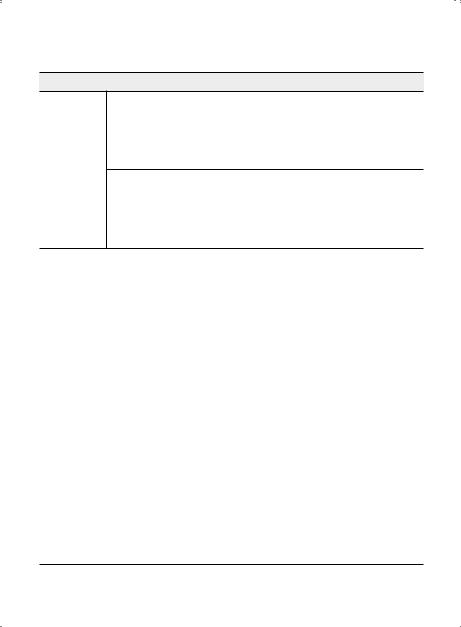
Table 5.10. Monitoring Plan During Treatment for HCV Infection |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Weeks of Treatment |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Baseline |
2 |
4 |
|
8 |
12 |
|
16 |
|
20 |
24 |
24–28 |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CBC |
X |
|
X |
X |
|
X |
|
X |
|
X |
|
X |
X |
q4 weeks |
LFTs + metabolic |
X |
|
|
X |
|
X |
|
X |
|
X |
|
X |
X |
q4 weeks |
panel |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HCV RNA |
X |
|
|
X¶ |
|
|
|
X* |
|
|
|
|
X** |
q12 weeks |
HIV RNA + CD4 |
X |
|
|
|
|
|
|
X† |
|
|
|
|
X |
q12 weeks |
profile |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TSH |
X |
|
|
|
|
|
|
X |
|
|
|
|
X |
q12 weeks |
Depression |
X |
|
X |
X |
|
X |
|
X |
|
X |
|
X |
X |
ongoing |
*Patients who have not dropped ≥2 logs from baseline HCV RNA at 12 weeks (early virologic response) have < 3% chance of obtaining a sustained viral response (undetectable HCV RNA 6 months post-treatment).. Optimally, the HCV RNA will be undetectable by week 12 (“complete” early virologic response).. One proposed strategy for patients with low-level detectable HCV RNA at week 12 (“partial” early virologic response) is to lengthen the course of therapy to 72 weeks or longer to reduce the risk of relapse; this is currently under investigation..
**If undetectable HCV RNA at 24 weeks, continue therapy for an additional 24 weeks (if known genotype 2 or 3 discuss option to stop, but some experts agree co-infected patients should continue treatment for 48 weeks to decrease risk of relapse).. If HCV RNA is positive at 24 weeks, consider discontinuing HCV therapy.. Even in patients without viral response, treatment may improve liver histology.. Also see Figure 5..1..
† |
Anticipate decrease in absolute cell count but stable CD4%.. |
¶ |
Check HCV RNA at week 4; if no decline in HIV RNA is seen, response is extremely unlikely.. In contrast, ≥ 1 log decline |
|
|
|
can be very motivating and treatment should be continued.. Best chance at cure is with an undetectable HIV RNA at |
|
4 weeks, sometimes called a “rapid virologic response..” |