

Chapter 6. Prophylaxis and Immunizations |
369 |
ENDOCARDITIS PROPHYLAXIS
Endocarditis prophylaxis is now recommended only for previous endocarditis, prosthetic cardiac valve or prosthetic cardiac valve material, congenital heart disease (CHD), unrepaired cyanotic CHD, including palliative shunts and conduits, completely repaired congenital heart defects with prosthetic material/devices (placed by surgery or by catheter intervention during the first 6 months post-procedure), repaired CHD with residual defects adjacent to the site of prosthetic patch/device, and cardiac transplantation with cardiac valvupathy.
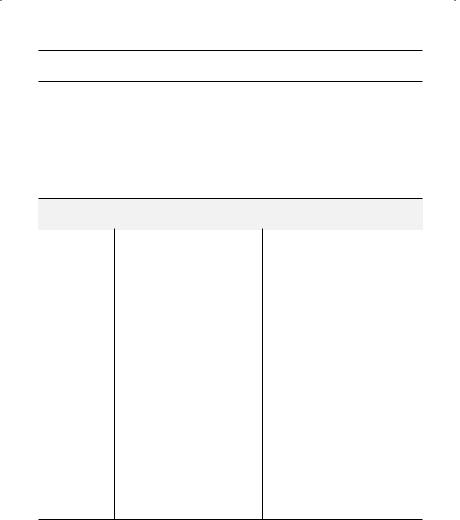
Table 6.9. Previous Indications for Infective Endocarditis (IE) Prophylaxis*
|
|
Prophylaxis Recommended |
|
Prophylaxis Not Recommended |
Subset |
|
(Column A) |
|
(Column B) |
|
|
|
|
|
Cardiac conditions |
• |
Ostium primum ASD |
• Isolated ostium secundum ASD |
|
|
• |
Prosthetic heart valves, |
• Surgical repair without residue |
|
|
|
including bioprosthetic and |
|
beyond 6 months of ostium |
|
|
homograft valves |
|
secundum ASD or PDA |
|
• |
Previous infective endocarditis |
• Previous coronary artery bypass |
|
|
• |
Most congenital cardiac |
|
surgery |
|
|
malformations |
• MVP without valvular regurgitation |
|
|
• |
Rheumatic valve disease |
• Physiologic, functional, or innocent |
|
|
• |
Hypertrophic cardiomyopathy |
|
murmurs |
|
• MVP with significant valvular |
• Previous Kawasaki’s cardiac disease |
||
|
• |
regurgitation |
|
or rheumatic fever without valve |
|
Calcific aortic stenosis |
|
disease |
|
|
|
|
|
|
Procedures |
• |
Dental procedures known |
• Dental procedures not likely to |
|
|
|
to induce gingival/mucosal |
• |
induce gingival bleeding |
|
|
bleeding, including dental |
Tympanostomy tube insertion |
|
|
|
cleaning |
• Flexible bronchoscopy ± biopsy |
|
|
• |
Tonsillectomy or |
• |
Endotracheal intubation |
|
• |
adenoidectomy |
• |
Endoscopy ± gastrointestinal |
|
Surgical operations involving |
• |
biopsy |
|
|
|
intestinal or respiratory mucosa |
Cesarean section |
|
|
• Cystoscopy or urethral dilation |
• D & C, IUD insertion/removal, or |
||
|
• |
Urethral catheterization or |
|
therapeutic abortion in the absence |
|
|
urinary tract surgery if UTI is |
• |
of infection |
|
• |
present |
Cardiac pacemaker/defibrillator |
|
|
Prostate surgery |
|
insertion |
|
•I & D of infected tissue
*Wilson W, et al.. Prevention of Infective Endocarditis.. Circulation 116:1736–1754, 2007..
370 |
A n t i b i o t i c E s s e n t i a l s |
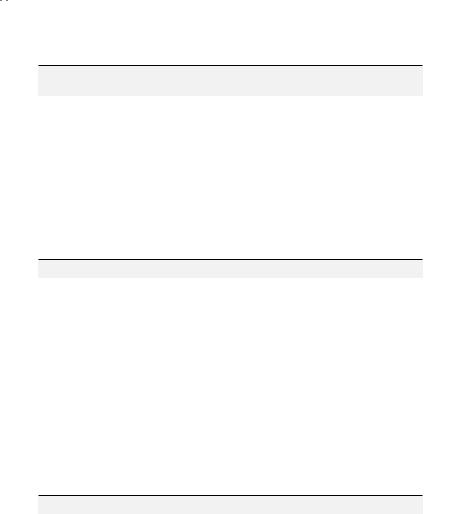
Table 6.9. Previous Indications for Infective Endocarditis (IE) Prophylaxis* (cont’d)
|
|
Prophylaxis Recommended |
|
Prophylaxis Not Recommended |
Subset |
(Column A) |
|
(Column B) |
|
|
|
|
|
|
|
• Biopsies of infected respiratory |
• |
Coronary stent implantation |
|
|
|
mucosa or infected skin/soft |
• |
Percutaneous transluminal coronary |
|
• |
tissues |
• |
angioplasty (PTCA) |
|
Any surgical procedure |
Cardiac catheterization |
||
|
|
involving an infected field |
|
|
|
|
|
|
|
ASD = atrial septal defect, D & C = dilatation and curettage, I & D = incision and drain, IUD = intrauterine device, MVP = mitral valve prolapse, PDA = patent ductus arteriosus, UTI = urinary tract infection.
*Prophylaxis is indicated for patients with cardiac conditions in Column A undergoing procedures in Column A.. Prophylaxis is not recommended for patients or procedures in Column B.. See Tables 6..9 and 6..10 for prophylaxis regimens for above-the-waist and below-the-waist procedures, respectively..
Table 6.10. Endocarditis Prophylaxis for Above-the-Waist (Dental, Oral, Esophageal, Respiratory Tract) Procedures*
Prophylaxis |
Reaction to Penicillin |
Antibiotic Regimen |
|
|
|
Oral prophylaxis |
None |
Amoxicillin 2 gm (PO) 1 hour pre-procedure† |
|
Non-anaphylactoid |
Cephalexin 1 gm (PO) 1 hour pre-procedure |
|
|
|
|
Anaphylactoid |
Clindamycin 300 mg (PO) 1 hour pre-procedure†† |
IV prophylaxis |
None |
Ampicillin 2 gm (IV) 30 minutes pre-procedure |
|
|
|
|
Non-anaphylactoid |
Cefazolin 1 gm (IV) 15 minutes pre-procedure |
|
|
|
|
Anaphylactoid |
Clindamycin 600 mg (IV) 30 minutes pre-procedure |
|
|
|
*Endocarditis prophylaxis is directed against viridans streptococci, the usual SBE pathogen above the waist.. Macrolide regimens are less effective than other regimens; clarithromycin/azithromycin regimens (500 mg PO 1 hour pre-procedure) are of unproven efficacy..
†Some recommend a 3 gm dose of amoxicillin, which is excessive given the sensitivity of viridans streptococci to amoxicillin..
††Some recommend a 600 mg dose of clindamycin, but a 300 mg dose gives adequate blood levels and is better tolerated (less diarrhea)..
Table 6.11. Endocarditis Prophylaxis for Below-the-Waist (Genitourinary, Gastrointestinal) Procedures Involving an Infected Field*†
Prophylaxis |
Reaction to Penicillin |
Antibiotic Regimen |
|
|
|
Oral prophylaxis |
None |
Amoxicillin 2 gm (PO) 1 hour pre-procedure |
|
|
|
|
Non-anaphylactoid, |
Linezolid 600 mg (PO) 1 hour pre-procedure |
|
anaphylactoid |
|
|
|
|