

25
Autogenous Bone Grafts in Maxillofacial Reconstruction
Michael Ehrenfeld and Christine Hagenmaier
Bone grafts in maxillofacial surgery are used to correct or replace missing bone. Bone defects can either be the consequences of congenital and developmental malformations or originate from tumor surgery, trauma, or infections. There are many indications for bone grafts in cosmetic surgery as well.
So far as the biological qualities of bone substitutes are concerned, fresh autogenous bone still represents the gold standard among all available grafting materials.1,2 Nonresorbable ceramic materials are prefered only for contour augmentation procedures because they do not have the unpredictable initial remodeling and resorption seen with free autogenous bone grafts.
Fresh autogenous bone grafts can be transplanted in three principally different techniques: free bone grafts, pedicled bone grafts, and microvascular bone grafts.3–19 For microvascular revascularized tissue transplants, some authors prefer the term “flap,” such as “the osteomusculocutaneous fibula flap.”
donor sites, free bone grafts with different bone qualities can be harvested.
Indications for Free Bone Grafts
Free bone grafts are generally indicated for the filling of bone defects, for example, after extirpation of large cysts. They are also used for ridge augmentation procedures in preprosthetic surgery and dental implantology. Small mandibular or maxillary continuity defects can be reconstructed with free bone grafts; other examples include osteotomy gaps in orthognathic surgery, defect zones in fractures, facial clefts, and small continuity defects in tumor surgery.33 Free bone grafts are also used for augmentation procedures in esthetic surgery (malar augmentation, chin augmentation), but because of a potential loss of bone volume, grafting materials with less resorption (nonresorbable ceramic implants, homogeneous cartilage) should be taken into consideration on a case-by-case ba-
sis.34,35
Free Bone Grafts
Free bone grafts are usually harvested from certain preferred donor site areas. During harvesting, tissue connections between bone graft and surrounding tissues are transected. In the recepient site the bone must be revitalized mainly via tissue ingrowth, although it is also known that osteocytes within free bone grafts are able to survive after transplanta- tion.1,2,20–26 The revitalization goes along with a process of initial remodeling and bone resorption, which is associated with a loss of bone volume. This process is generally called resorption. The amount of resorption depends on many factors, such as the dimensions of the bone graft (it takes longer to revitalize large bone grafts, and therefore they show a greater percentage of bone loss), the quality of the bone (cortical, cancellous), tissue qualities at the recipient site (vascularization), biomechanical properties (functional loading), and bone graft fixation to surrounding bone.7,27–32 A serious problem for the clinician is the fact that the amount of bone loss after free bone transplantation is unpredictable. From various
Donor Sites
The choice of the donor site depends on the amount as well as the desired quality of the bone and potential donor site morbidity. The patients also must be informed about alternatives.
Chin
From the chin of mandibles of normal height, cortical bone grafts and also some cancellous bone can be taken in an amount of 3 cm3.36,37 The exposure of the chin region is performed from an intraoral incision. Depending on the patient’s dentition, the incision is made in the nonattached vestibular mucosa or at the junction of the gingival margin. Under the apices of the lower incisors and canines and laterally to the mental foramina, the vestibular cortical plate is cut with a small round bur or a microsaw and taken with the use of a chisel (Figure 25.1). Under the cortical plate, some cancellous bone is also available. The amount of bone is sufficient for smaller regional grafting procedures such as cleft osteo-
295

296
FIGURE 25.1 Harvesting of bone grafts from the chin.
plasties, filling of osteotomy gaps, and regional augmentation procedures in implantology. If a large bone graft has been taken, the defect in the chin region should be filled with resorbable ceramics or covered with a semipermeable membrane (guided bone regeneration) to prevent supramental soft tissue depression. The harvesting of too much cancellous bone can result in a permanent devitalization of the anterior mandibular dentition.
Retromolar Area
From the retromolar regions of both mandible and maxilla, small cortical and corticocancellous bone grafts can be taken via intraoral incisions and without significant donor site mor-
M. Ehrenfeld and C. Hagenmaier
FIGURE 25.3 After a small incision in the upper vestibule, free bone graft can be taken from the nasal aperture.
bidity (Figure 25.2).38 The access is not as easy compared to the chin, and the amount of bone is somewhat smaller. It can be used for the same indications as bone grafts from the chin. One should consider the retromolar regions if the patient’s wisdom teeth need to be removed.
Nasal Aperture
A small amount of cortical bone can be taken from the nasal aperture via an intraoral incision in the upper vestibular mucosa (Figure 25.3). Other than swelling and pain for a few days, there is no donor site morbidity. The bone is sufficient for small defects such as localized ridge augmentations in dental implantology.
FIGURE 25.2 Retromolar area of the mandible is exposed for harvesting of free nonvascularized bone grafts.
Skull
From the skull, full-thickness free bone grafts as well as splitthickness cortical bone grafts from the outer table can be har- vested.39–41 Full-thickness bone grafts are taken for skull reconstruction. They are harvested using a template and then split with the help of a saw and a chisel in two grafts, one representing the outer and the other the inner table. One is used to reconstruct the missing bone, and the other is replanted into the donor site defect to reestablish normal contours and brain protection.
Outer table bone grafts can be harvested as cortical bone grafts of varying thickness, and as thicker corticocancellous bone grafts as well. Especially in craniofacial traumatology, calvarial bone grafts have become widespread in use, but they are also used in preprosthetic and esthetic surgery. The skull is exposed through a coronal or hemicoronal incision; the patient’s head is not shaved (Figure 25.4). The bone is usually taken posteriorly from the coronal and laterally from the sagittal suture. To avoid injury to the sinuses and massive hemorrhage, care must be taken to place the donor site in such a way as to prevent perforation of the inner table in these areas.

25. Autogenous Bone Grafts in Maxillofacial Reconstruction |
297 |
FIGURE 25.4 Planning of a coronal incision. The patient’s hair has been treated with a gel, and then the incision line is defined with a comb. After that the head is washed with a local disinfectant.
After exposure of the bone surface the desired size and shape of the bone graft are marked with a round bur (Figure 25.5). Drilling is performed through the outer table until a decreasing resistance indicates that the bur has reached the diploe. After that, a microsaw is inserted underneath the cortical bone to free it from the diploe (Figure 25.6). The osteotomy is then completed with a small chisel (Figures 25.7, 25.8). The use of a microsaw before introducing the chisel significantly reduces the risk of unpredictable fractures of the bone graft. Significant bleeding from the well-perfused diploe is prevented using bone wax to seal the donor site vessels. Harvesting of outer table bone grafts can result in a palpable depression, which is usually hidden to the observing eye. Nevertheless, the donor site defects can be filled with a pericranial galeoperiosteal rotation flap or alloplastic materials (ceramic implants, GoreTex sheets). Serious complications may arise from perforations through the inner table with subsequent hemorrhage and all the possible sequelae of epidural or, in extreme cases with dural laceration, subdural hemorrhage.
FIGURE 25.6 A microsaw is introduced between cortex and diploe to separate the table.
FIGURE 25.7 The bone graft is mobilized with the help of a small chisel.
FIGURE 25.5 The desired amount of bone is marked. With a bur, the outer cortex is divided until the diploe is reached.
FIGURE 25.8 Isolated bone graft from the outer table for reconstruction of facial walls.
298 |
M. Ehrenfeld and C. Hagenmaier |
Rib
A free rib graft was among the first autogenous bone grafts to reconstruct the continuity of a mandible.6,7,42 Because of the insufficient amount of bone and unpredictable resorption, a free rib graft today is not among the bone grafts of choice for mandible reconstruction in adults. Free rib grafts can be harvested at full thickness or split thickness and as composite costochondral grafts. Today we rarely see an indication for a fullor split-thickness rib graft, whereas costochondral grafts are used for reconstruction of the ascending ramus in children and for the condylar process in adults. A rib segment is harvested from a slightly curved incision in the anterior chest wall on the right side (Figure 25.9). Normally the fifth, sixth, or seventh rib, and in special cases also more than one rib, are taken. The incision is performed through skin and subcutaneous tissue and through the attached muscles to the anterior rib surface. After that the periosteum is stripped and the
FIGURE 25.10 After stripping of muscles and periosteum the rib is osteotomized, in this pediatric patient with a help of a microsaw. The underlying soft tissues and the pleura must be protected.
osteotomies are performed with a saw or a special rib cutter (Figure 25.10).
Care must be taken not to harm the pleura. If a pleural laceration occurs, the defect must be sutured and a control x-ray must be taken after the operation because a pneumothorax may result. In the treatment of a possible pneumothorax, a thoracic surgeon should be consulted. Another possible complication is the development of pleuritis. The left side of the chest wall should be avoided to prevent penetration of the pericardium. After harvesting a rib graft, patients often complain of uncomfortable pain associated with movements of the chest wall while breathing.
FIGURE 25.9 Free rib grafts are taken after a slightly curved incision overlying the fifth, sixth, or seventh rib on the right side of the chest wall. In female patients, the incision line can be hidden in the breast fold.
Iliac Crest
The iliac crest is a donor site of outstanding importance for all kinds and shapes of free bone grafts and vascularized bone flaps.9,43–45 Bone from the hip can be taken as cancellous, thin cortical, corticocancellous, and bicorticocancellous (fullthickness) bone grafts. The bone can be taken from the anterior iliac crest posteriorly to the anterosuperior iliac spine or the posterior ilium. The anterior iliac crest is the donor region of choice in most cases because during maxillofacial operations patients are usually in a supine position. To approach the posterior ilium a patient must be turned and thus the operation is prolonged; also, two-team operations are not possible. The size and the form of the ilium permits creating bone grafts in different shapes and sizes. The different bone grafts and bone qualities from the hip cover all the indications for free bone grafts as listed here.
Cancellous bone can be harvested as particulate bone and marrow and as cancellous bone blocks. To avoid donor site complications, cancellous bone and marrow are best taken utilizing a fenestration technique. The iliac crest is approached by a skin incision along the iliac bone with the muscles attached to the lateral side of the ilium remaining untouched.

25. Autogenous Bone Grafts in Maxillofacial Reconstruction
FIGURE 25.11 In pediatric patients the cartilage overlying the bony part of the ilium is separated from the bone with a scalpel. No osteotomy is needed for harvesting of cancellous bone and marrow.
In an adult, the fascia overlying the iliac crest is incised including the periosteum, with the periosteum and the muscles stripped only from the upper border of the iliac crest. With a saw, the cortical plate is cut but remains attached to the medial periosteum and the attached muscles. The marrow is harvested with a sharp spoon curette. After that, the cortical plate
299
is repositioned and fixed with a strong resorbable suture. With this technique the lateral and medial muscles stay in place and the bony contour is not affected. In pediatric patients, the cartilaginous growth area overlies the bony iliac crest and should be preserved to avoid growth disturbances and deformations of the hip. After exposure of the hip as described, the cartilage is separated from the bone with a knife (Figure 25.11). The bone under the cartilage is soft and can be harvested without any problems. Then, the cartilage is repositioned and fixed with a resorbable suture. Generally the wounds must be closed layer by layer.
Cancellous bone blocks are harvested with a similar technique, but in addition the periosteum on the inner surface of the hip must be elavated to allow an osteotomy of the inner cortex. The cortex on the lateral surface of the ilium is usually thin and is included in a cancellous bone block (Figure 25.12). The segment is then mobilized with a saw and a chisel and subsequently removed. The inner cortex is drilled down if a purely cancellous block is desired. A small amount of cancellous bone can also be taken through a stab incision laterally or above the iliac crest with the help of a trephine.
Cancellous bone and marrow are used to fill bone defects after extirpation of bone cysts, for alveolar clefts, and for smaller continuity defects such as defect fractures or osteotomy gaps. For reconstruction of larger continuity defects, cancellous bone and marrow were used in the past in tray systems such as titanium or dacron meshes or even in homogeneous mandibular cribs. Recent publications report significant complication rates after continuity reconstructions with cancellous bone and marrow in titanium trays.46,47 In the authors’ experience microvascular bone flaps are far superior to cancellous bone in tray systems, especially for reconstruction of larger continuity defects and in donor sites of poor quality.
In preprosthetic surgery, cancellous bone from the hip is used for sinus augmentation procedures and in combination with semipermeable membranes for localized ridge augmen-
FIGURE 25.12 Cancellous bone blocks from the hip are removed from the inner surface with the inner cortex in place during harvesting.

300
tations. Cancellous bone blocks are frequently used for onlay and interposition osteoplasties in preprosthetic surgery and for reconstruction of (smaller) mandibular or maxillary continuity defects in jaw reconstruction or in complex orthognathic operations. Some authors prefer cancellous bone blocks versus corticocancellous bone grafts because for new bone formation the cortical layer-barrier is missing; other authors prefer corticocancellous grafts because of fixation reasons. Screws tend to have more primary stability if they engage at least one cortex, although the cortical part of the graft primarily is not vital bone.
Corticocancellous bone grafts are best taken from the inner surface of the hip, because the stripping of the inner periosteum is not as painful as the stripping of the outer periosteum, especially during walking on the first postoperative days. The approach is similar to that described for cancellous bone and marrow. In addition, the periosteum on the medial aspect of the ileum is elevated, including the attached muscles of the abdominal wall. With the help of a saw and a chisel, corticocancellous bone grafts can be harvested without contour deformations. As described, corticocancellous bone grafts mainly cover the same range of indications as cancellous bone blocks.
If a bicorticocancellous bone graft is needed, the periosteum and muscles must be stripped on both the inside and outside of the hip. Contour deformations can be avoided if the iliac crest itself is preserved (Figure 25.13). Bicortical grafts are sometimes used for mandibular reconstruction because they are more easily fixed with plates and screws than are cancellous blocks. After the fixation of a bicortical graft, the cortex areas not used for bone graft fixation should be
FIGURE 25.13 Harvesting of a bicorticocancellous bone block should be performed with preservation of a bony bridge in the region of the iliac crest to prevent contour deformations.
M. Ehrenfeld and C. Hagenmaier
perforated with multiple bur holes or drilled down for better tissue ingrowth.
The hip is not the donor site of first choice for cortical bone grafts. Cortical bone grafts are mainly used in complex craniofacial surgery. These cases are frequently approached via a coronal incision, and thus the outer table of the skull, which is an excellent donor site for bone grafts, is already exposed. Also, the cortical plates of the hip are very thin and sometimes very soft. Complex craniofacial osteotomies sometimes require cancellous bone and cortical bone grafts as well, and in these rare cases both can be taken from the hip.
Tibia
In adult individuals, cortical and corticocancellous bone grafts can be harvested from the anterior surface of the tibial plateau without significant donor site complications. Bone grafts from the tibia have been used mainly for ridge augmentation and cleft palate procedures.
Pedicled Bone Grafts
In contrast to free bone grafts, pedicled bone grafts remain connected with the donor site by a vascular pedicle or attached soft tissues. This requires that the donor and recipient sites be located close to each other.
Pedicled Rib Grafts
Vascularized rib grafts can be harvested together with a pectoralis major muscle flap (vascular pedicle: superior thoracoacromial vessels) and in combination with a latissimus dorsi flap (vascular pedicle: branches from the thoracodorsal vessels to the serratus anterior muscle and the anterior chest wall). Both types of combined musculocutaneous-osteocutaneous flaps have been used for simultaneous reconstruction of large soft tissue defects in combination with continuity defects of the mandible.17,18,48 Because of the limited range of these flaps, their indication is mainly limited to tissue defects in the lower third of the face and the neck with accompanying defects of the mandible. Today pedicled rib grafts together with soft tissue flaps from the pectoralis major or latissimus dorsi muscle are not the grafts of first choice, especially for mandible reconstruction, because the perfusion of the rib is unpredictable and pedicled rib grafts are often lost because of infection or partially lost because of resorption. Besides that, a rib usually does not give enough volume for functional mandible reconstruction. The placement of dental implants is virtually impossible.49 In the authors’ opinion, the current indications for combined pedicled flaps are limited to special problems in reconstruction, which in our hands consist mostly of large soft tissue defects in patients who have had radical cancer operations in the lower facial third and neck with fulldose irradiation therapy.

25. Autogenous Bone Grafts in Maxillofacial Reconstruction
Temporalis Osteomuscular Flap
Together with the well-known temporalis muscle (better, musculofascious) flap, pedicled on the deep temporal vessels, a splitor even full-thickness portion of underlying temporal bone can be harvested. In connection to the temporal vessels the composite flap has a limited range and limited freedom of orientation as well, but it has been used to reconstruct maxillary and hard palate defects and even segments of the ascending mandibular ramus. The composite flap has also been advocated for use as a free microvascular flap, but poor results have been reported, especially for mandible reconstruction.50
Harvesting of temporal muscle and composite flaps may have a significant donor site morbidity. Among the unwanted side effects are a temporary or even permanent reduction in mouth-opening capacity and an unpleasant cosmesis known as temporal hollowing. The latter can be camouflaged by implanting alloplastic material (silastic, Gore Tex, ceramics, or other) into the temporal region.
Microvascular Bone and Composite Flaps
Microvascular bone flaps are always combined hard and soft tissue composite grafts, with bone, periosteum, and attached muscles, the so-called osteomuscular flaps. These composite flaps can be harvested from several donor areas; most frequently used in craniomaxillofacial reconstructive bone surgery are flaps from the iliac crest, scapula, fibula, and forearm. Composite bone grafts with a skin island are called osteomusculocutaneous flaps. In contrast to free nonvascularized grafts, microvascular bone flaps are nourished over a vascular pedicle containing a supplying artery and at least one draining vein, which in the recipient site must be connected to an artery and one or two accompanying veins. Under ideal conditions a microvascular flap therefore remains viable tissue directly after transplantation and does not need to be revascularized from the surrounding tissues. As an important consequence, almost no initial bone resorption and bone loss are observed after transplantation. A microvascular flap is by far more independent from the tissue qualities in the recipient site (scar formation, previous irradiation) compared to nonvascularized grafts. The possibility of transferring soft tissues together with bone for combined one-stage bone and soft tissue reconstruction has advantages in tumor surgery.
In contrast, a microvascular bone transplantation is technically much more demanding than a free bone transfer. It requires special surgical training and special equipment. Microvascular tissue transplantations are usually lengthy operations and can be problematic for patients in poorer general condition.
Indications for Microvascular Boneflaps
Microvascular bone flaps are indicated for the reconstruction of large bone defects, defects in recipient sites of poor qual-
301
ity, and when a simultaneous bone and soft tissue reconstruction is desired.
Combined Iliac Bone and Soft Tissue Flaps
Osteomuscular bone flaps from the hip contain iliac bone, periosteum, and at least a small strip of iliac muscle. Additional larger muscle islands from the internal oblique muscle are also possible. Both types of transplants can be harvested pedicled at the superficial circumflex iliac artery and vein (SCIA, SCIV) and the deep circumflex iliac vessels as well (DCIA, DCIV). The DCIA and DCIV are the more reliable vessels as far as the blood supply of the various iliac flap modifications is concerned.16
Iliac bone flaps are raised with the patient in a supine position and the donor site hip is elevated with the help of a cushion. The superior iliac spine, the iliac ligament, the pubic bone, and the femoral artery are palpated and marked on the patient’s skin (Figure 25.14). The DCIA leaves the external iliac artery on its medial aspect normally 1 to 3 cm cranially to the inguinal ligament. The venous blood is usually drained by two accompanying veins, which mostly form one venous trunk 1 to 2 cm before the external iliac vein is reached. The two veins have complex connective branches and sometimes resemble a network of more than two distinct vessels. Therefore, both veins must be preserved during dissection. The DCIA and accompanying veins run superior to the inguinal ligament in a duplication of the fascias of the thigh and the abdominal wall, and reach the inner aspect of
FIGURE 25.14 The femoral artery, the inguinal ligament, and the iliac crest are palpated and marked. The supplying vessels (DCIA, DCIV) leave the external iliac artery superior to the inguinal ligament toward the medial aspect of the iliac crest. The axis of the skin portion should be parallel to the crest; two-thirds of the skin island is located superiorly to the bone margin. The level of the perforators is outlined with dots.

302
FIGURE 25.15 The femoral artery and vein are identified. After that the skin overlying the inguinal ligament is incised and the junction of the fascias of the abdominal wall and the thigh is exposed. The inguinal ligament is cut parallel to the axis of the DCIA and DCIV.
the ilium in the fascia of the iliac muscle 1 to 3 cm from the inner cortex of the iliac crest.
Overlying and superior to the iliac crest a skin island can be harvested. The skin portion is nourished by perforating vessels from the DCIA and DCIV, which reach the surface on the medial aspect of the iliac crest at a distance of 1 to 2 cm. The axis of the skin flap lies between the superior inferior iliac spine and tip of the scapula. Dissection starts with the exposure of the femoral artery, which can be easily palpated caudally to the inguinal ligament. Further dissection in the proximal direction leads to the DCIA, which leaves on the lateral aspect of the vessel, now called the external iliac artery, normally 1 to 3 cm cranially to the inguinal ligament (Figure 25.15). After that the DCIA and frequently the two accompanying veins are dissected as a bundle in a craniolateral direction. Dissection comes to a stop at 2 to 3 cm from the anterior superior iliac spine (Figure 25.16).
To raise an osteomuscular bone flap with a skin island, the desired skin portion is now dissected free. The incision divides skin and subcutaneous tissues down to the underlying abdominal fascia. Medially to the anterior superior iliac spine,
M. Ehrenfeld and C. Hagenmaier
FIGURE 25.17 The edges of the skin island are cut down to the underlying fascia after the vascular pedicle has been isolated. The three layers of the abdominal muscles are divided leaving a muscle strip 3 cm wide attached to the bone and the overlying skin. The vascular pedicle lies in the junction of the iliacus and the transversalis fascia.
the lateral cutaneous femoral nerve should be exposed and preserved. The external and internal oblique as well as the transverse abdominal muscles are now incised 3 to 4 cm cranially to the iliac crest (Figure 25.17). The muscle portion of the flap must remain attached to the fascia and the skin so as not to harm the blood supply of the skin. The strip of abdominal muscle attached to the medial aspect of the iliac crest contains the perforating vessels, which are very sensitive and may be harmed even by shearing the different soft tissue layers against each other. At 3 to 4 cm superior to the iliac crest, the transverse abdominal muscle is represented through the transverse fascia, which is also incised. The abdominal wall is retracted medially, and the junction between transversal fascia and the fascia of the iliac muscle is identified (Figure 25.18). The vascular pedicle lies in the duplication of the two fascias and can be palpated at this stage.
The muscles on the lateral aspect of the ilium are then stripped. The periosteum can either be elevated or left in place if additional soft tissue coverage of the bone is desired. The
FIGURE 25.16 The vascular pedicle containing the DCIA and in most cases two accompanying veins is dissected.
FIGURE 25.18 The fascia of the iliacus muscle together with a 2- to 3-cm strip of muscle must also be included in the flap. The iliacus muscle can be divided by blunt dissection.
25. Autogenous Bone Grafts in Maxillofacial Reconstruction
bone is then osteotomized with an oscillating saw in the desired size and shape (Figure 25.19). The osteotomy site is sealed with bone wax (Figure 25.20). The iliac bone flap is completely freed from all surrounding tissues and remains only connected to the vascular pedicle. If there is any delay in the craniofacial part of the operation (tumor ablation, preparation of the recipient site), the flap is deposited in a subcutaneous pocket. Shortly before transplantation, the DCIA and then the DCIV are ligated and transected. The flap may be irrigated with saline solution but is not routinely rinsed with anticoagulants.
For raising of an osteomuscular iliac bone flap without a skin or a separate muscle island, the dissection is performed very similarly to the procedure just described. Because no skin is taken, the abdominal skin overlying the iliac crest is incised parallel to the bone. On the medial aspect of the ilium, the transverse and oblique abdominal muscles are cut close to the bone; only a strip of iliac muscle and fascia containing the vascular pedicle is left attached to the medial aspect of the ilium.16,51,52
A special consideration, in obese patients, is that the composite osteomusculocutaneous iliac bone flap provides too much bulk for intraoral soft tissue reconstruction. As an important variation, a osteomuscular flap with a large fasciomuscular soft tissue island from the internal oblique muscle can be harvested.53 Therefore, the fascia of the transverse abdominal and external oblique muscles is cut close to the iliac crest. The internal oblique, underlying the external fascia and muscle, is now exposed. A nonconstant separate branch of the DCIA, which leaves the artery on its way between the internal iliac artery and anterior superior iliac spine, may go directly to the internal oblique muscle in a mediocranial direction and should be preserved when present. The internal oblique muscle and its fascia are dissected in the desired length and remain attached to the medial aspect of the iliac crest. A strip of iliac muscle containing the vascular pedicle is also included in the flap. The result is a compound flap of solid iliac bone with a potentially large soft tissue island of
303
FIGURE 25.20 The vascular pedicle is ligated and divided after complete isolation of the flap. After sealing the iliac bone with bone wax, the abdominal wall is closed layer by layer.
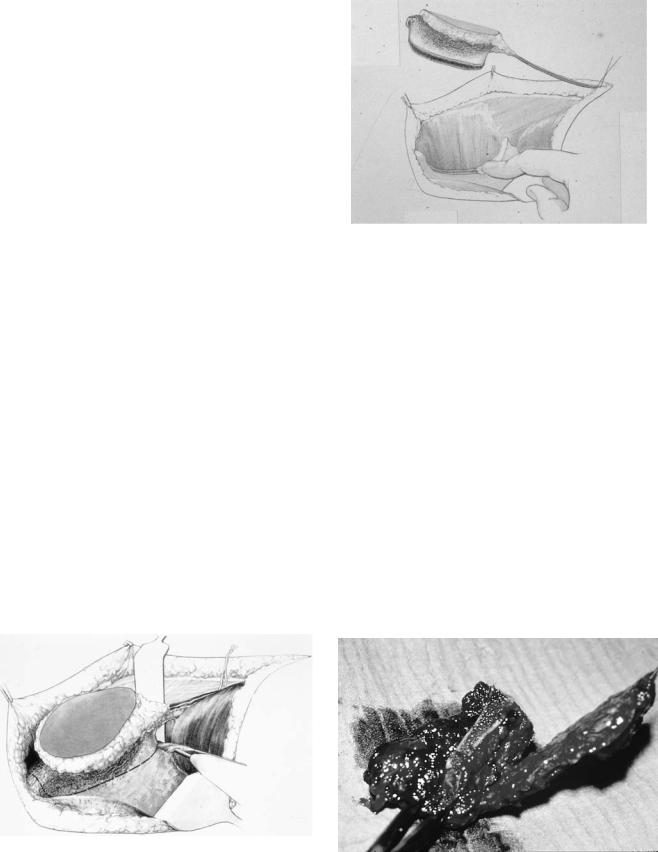
internal oblique muscle and fascia (Figure 25.21), which can be used to replace resected intraoral mucosa (Figure 25.22). Therefore, the intraorally placed muscle and fascia are left to granulation (Figure 25.23) and subsequent secondary epithelialization from the surrounding mucous membrane. Despite a certain amount of shrinkage, usually good functional results can be obtained (Figure 25.24).
Flap Contouring
Especially in chin reconstruction, the only slightly curved iliac bone must be bent to adapt it to the shape of a mandible. For this purpose, the outer cortex (lateral cortex) of the flap’s bony portion is osteotomized with an oscillating saw (Figure 25.25). The bone cut goes through the outer cortex and the cancellous portion of the flap. Care must be taken not to penetrate the medial cortex, because in so doing the attached segment of iliac muscle, the periosteum, and the vascular pedi-
FIGURE 25.19 After stripping of muscles and periosteum attached to |
|
the lateral aspect of the iliac crest, the bony portion is cut with an |
FIGURE 25.21 Osteomuscular bone flap from the hip with attached |
oscillating saw. |
internal oblique muscle. |

304 |
M. Ehrenfeld and C. Hagenmaier |
FIGURE 25.22 The internal oblique muscle can be used to cover defects of the oral mucosa, in this clinical case, of the anterior floor of the mouth.
FIGURE 25.25 An osteotomy of the former lateral cortex of the hip now included in osteomuscular iliac bone flap is necessary if the bone must be bent to adjust it to a special clinical situation.
cle may be injured, thus compromising the blood supply. After that the bone can be bent in the desired fashion (Figure 25.26).
Scapular Bone and Combined Flaps
The scapula is a triangular-shaped bone with a very thin center portion, whereas the borders of the scapula are composed of more solid bone. The lateral border of the scapula provides sufficient bone for craniomaxillofacial reconstruction purposes. Pedicled on the circumflex scapular artery and frequently two accompanying veins, bone flaps with a thickness of approximately 1.5 cm, a height of approximately 3 cm, and a length of 10 to 14 cm can be harvested. Although the
FIGURE 25.23 The muscle granulates after transplantation and is secondarily epithelialized from the surrounding mucosa.
FIGURE 25.24 Clinical situation after the granulation process is finished.
FIGURE 25.26 Bone flap after multiple monocortical osteotomies. Depending on the desired length of the flap, the bone can either be contoured by removing wedges from the lateral aspect of the hip or by monocortical osteotomies and bending to the medial aspect as shown. The bone gaps at the osteotomy sites are then filled with cancellous bone and marrow.

25. Autogenous Bone Grafts in Maxillofacial Reconstruction
absolute amount of bone depends very much on the individual patient’s condition, the lateral border of the scapula is usually composed of enough bone even for mandible reconstruction.
The vascular axis containing the circumflex scapular artery can be elongated in dissecting the subscapular vessels up to the axilla. Through this technique a long vascular pedicle of approximately 12 to 14 cm can be created, which has advantages for special indications, among them reconstruction of the maxilla or mandible in a compromised vessel situation. On the common subscapular vascular pedicle, the scapular bone flap can be combined with a scapular or parascapular fasciocutaneous and a musculocutaneous flap from the latissimus dorsi muscle. Various flap combinations are also possible.
Flap dissection is usually performed with the patient turned on their side. Important anatomic landmarks are the scapular spine, the lateral border of the scapula, and the muscle gap between major and minor teres muscles on one side and the long triceps head on the other side. This muscle gap lies cranially to the middle portion of the lateral margin of the scapula. The bone is supplied via vessels running in a deep plane parallel to the lateral margin of the bone, whereas two other small terminal branches of the circumflex scapular artery nourish the scapular and parascapular flaps, respectively (Figure 25.27). The scapular flap is raised over a vascular axis that runs parallel to the scapular spine approximately in the middle between scapular tip and scapular spine. The parascapular flap vessel axis also lies parallel to the lateral margin of the scapula, but in a subcutaneous plane.
FIGURE 25.27 Bone grafts from the glenoid fossa to the tip can be taken from the lateral aspect of the scapula. Pedicled on the cutaneous branches of the circumflex scapular artery, a scapular or parascapular skin flap (or both) can be harvested in addition. Before dissection of the lateral border of the scapula, the crista scapulae and the muscular gap between teres minor and major muscles and the long head of the triceps muscle are palpated and marked.
305
To make microvascular anastomoses easier, it is advisable to include the subscapular artery and vein in the pedicle and therefore prepare as much vessel length as possible. The dissection of the axillary and subscapular vessels starts with a skin incision over and parallel to the anterior axillary fold. In the loose subcutaneous tissues, the junction between axillary and subscapular vessels is exposed. The circumflex scapular artery leaves the subscapular artery normally 2 to 4 cm caudally to the axillary vessels. As an important variation, sometimes both arteries leave the axillary artery separately. Two veins normally run with the circumflex scapular artery; both should be dissected and preserved. The vascular pedicle is further dissected medially into the lateral muscular gap. Careful ligation of small vessels to the surrounding muscles is mandatory. To gain better access, the skin overlying the vascular pedicle can be incised. The muscle gap beside the lateral scapular border is palpated and localized. After retraction of the latissimus dorsi and teres major muscles, the vascular pedicle can be seen in the muscle gap. There the subscapular vessels divide into three terminal branches, one to the bony portion and the remaining two to the scapular and parascapular skin islands.
If a combination of a bone flap together with a scapular or a parascapular flap is desired, the size of the soft tissue island must be defined at that stage of the operation. This is usually performed with the help of an individual template. Then, an incision is made through skin and underlying fascia and the soft tissue flap is raised from the muscle. This is performed from medially to laterally in the case of the scapular and in a caudal-cranial direction so far as the parascapular flap is concerned. Lateral to the bony border, in the region of the muscle gap, both skin flaps must remain in connection with the circumflex scapular vessels.
If a osteomuscular bone flap without additional skin flaps is desired, the skin overlying the scapula is simply incised parallel to the lateral bone margin from the scapular spine to the tip. On the lateral aspect of the scapula, the teres minor muscle inserts cranially and the teres major muscle inserts caudally. The muscles are cut leaving a muscle strip at least 1 cm wide attached to the bone. The vascular pedicle is thus protected. Osteotomy of the bone is now performed from posterior with a saw (Figure 25.28). The upper osteotomy line must remain approximately 2 cm from the glenoid fossa. Now the one strut, which is still connected to the underlying muscles, is elevated.
The subscapular muscle, which has its origin on the costal aspect of the scapula, is incised leaving a muscle strip of approximately 1 cm attached to the bone. The bone or combined bone and soft tissue flap is now completely isolated on its vascular pedicle, and the latter is ligated in the desired length (Figure 25.29). If the subscapular vessels are included in the vascular axis, the thoracodorsal artery and vein must also be ligated. Preserving these vessels allows various flap combinations potentially including a scapular bone flap, scapular and parascapular soft tissue flaps, and

306 |
M. Ehrenfeld and C. Hagenmaier |
FIGURE 25.28 After dissection of the circumflex scapular vessels, and, if a long vascular pedicle is required the subscapular vessels as well, the desired fasciocutaneous flap is elevated first. The muscles attached to the lateral border of the scapula are then divided leaving a strip of muscle approximately 2 cm wide attached to the bone. The muscles inserting on the posterior aspect of the scapula are also divided, leaving a thin muscle cuff in place. The bone is cut with a saw and elevated. After access is given to the costal surface of the scapula, the subscapular muscle is divided.
a musculocutaneous latissimus dorsi flap,19,51,52 (Figure 25.30).
Fibula Bone and Combined Flaps
The fibula is a source for long bone flaps with a compact bone structure. The flap can be harvested with the patient lying on the back, side, or abdomen. A two-team approach in max-
FIGURE 25.29 The osteomuscular and the fasciocutaneous portions of the combined flap are isolated and pedicled on the common vascular axis represented by the circumflex scapular vessels. The latissimus dorsi muscle is elevated. Now the flap can be transposed anteriorly into the axilla, and the subscapular vessels can be dissected to gain a longer vascular pedicle. An additional portion of a latissimus dorsi flap pedicled on the thoracodorsal vessels can also be included in the flap.
FIGURE 25.30 Combination of osteomuscular and fasciocutaneous scapula and a musculocutaneous latissimus dorsi flap on the common subscapular vascular pedicle.
illofacial reconstructive surgery can usually only be achieved with the patient in a supine position. The patient’s leg is flexed in both hip and knee with the hip joint in inward rotation. In this position the complete fibula can normally be palpated through the skin from the fibula head to the lateral malleolus (Figure 25.31).
The supplying vessel of the fibula bone and combined flap is the peroneal artery, which rarely is also the dominant vascular supply for the foot. Therefore, before flap harvesting an angiogram is mandatory. The vascular axis of the bone flap lies medial to the fibula. The bone itself is nourished mainly via perforators to the medial periosteum. As a consequence, stripping of the medial periosteum during dissection or flap fixation must be avoided. Dissection of the bone flap starts with the incision of the skin on the lateral aspect of the fibula.
FIGURE 25.31 For harvesting of a fibula flap, the patient’s leg is flexed in both hip and knee with the hip joint in inward rotation. In this position the complete fibula is palpated through the skin from the fibula head to the external malleolus and marked. An ovally shaped skin island can be harvested parallel to the bone axis and overlying the proximal two-thirds of the bone.

25. Autogenous Bone Grafts in Maxillofacial Reconstruction
The common popliteal nerve, which runs in a subcutaneous plane lateral to the fibular head, is exposed and preserved. The subcutaneous tissues are separated down to the deep muscular fascia. After that, the so-called posterior intermuscular septum between the anteriorly (long and short peroneal muscles) and posteriorly located muscles (soleus muscle, long and short flexor hallucis muscles) is dissected (Figure 25.32). Blunt dissection of the anteriorly and posteriorly located muscles gives good access to the lateral surface of the fibula. The peroneal muscles are freed from the fibula, whereas the periosteum should remain attached to the bone because stripping of the lateral periosteum may lead to an elevation of the periosteum on the medial side, thus separating the vascular pedicle from the bone. Preservation of the periosteum is essential for the blood supply to the bony portion of the flap.
This first step of the dissection ends when the anterior edge of the fibula is reached. Adherent to the anterior edge is the anterior intermuscular septum. It is cut close to the bone, and then the long and short extensor digitorum muscles are also separated from the bone again in an epiperiosteal plane. Directly in front of the fibula, the anterior tibial artery and vein can be palpated and inspected after the extensor muscles have been cut. These vessels must be preserved; together with the extensor muscles they are retracted to the side. The interosseous membrane is exposed over and cut shortly above the fibula. The vascular axis of the fibula flap containing the peroneal vessels, lying on the medial aspect close to the bone, must be handled with great care. Now the fibula is osteotomized in the desired length to allow sufficient access to the soft tissues on the posteromedial side of the bone (Figure
FIGURE 25.32 Cross cut through the lower leg. The supplying peroneal vessels are lying on the medial aspect of the bone. The skin island is nourished by perforators from the peroneal vessels, which come around the posterior surface of the fibula into the posterior intermuscular septum. Sometimes they are lying in the soleus muscle close to the muscle surface. Therefore, some authors recommend including a strip of soleus muscle in the flap.
307
FIGURE 25.33 Harvesting of a bone-only flap. After detaching the muscles on the lateral and anterior surface of the fibula, the bone is divided and transposed laterally. After that the peroneal vessels are easily identified. A strip of the posterior tibialis and hallucis longus muscles together with the periosteum remains attached to the bone.
25.33). The bony segment is mobilized laterally and posteriorly. Behind the distal osteotomy line the peroneal vessels are identified and ligated. The vascular pedicle lies posterior to the interosseous membrane embedded in loose connective tissues. In this stage of the dissection, care must be taken to not separate the vessels from the periosteum. Finally, the peroneal vessels are dissected proximally up to the popliteal vessel and then ligated.
If a fibula flap with a skin paddle is required, the planning starts with the definition of the desired amount of skin. The axis of the skin portion overlies the lateral border of the fibular bone and the posterior intermuscular septum. Blood supply to the skin is brought by septocutaneous or musculocutaneous perforators out of the peroneal vessels, which are located in the posterior intermuscular septum and sometimes in the soleus muscle close to the muscle surface. To make perfusion of the skin island safer, it is recommended that a strip of soleus muscle adjacent to the intermuscular septum be included in the flap.
The posterior and anterior edges of the flap are incised and the skin is elevated on both sides together with the deep fascia. Via the posterior intermuscular septum, the center of the flap always remains in close contact to the lateral aspect of the bone. The skin portion is now elevated anteriorly and the dissection is directed toward the posterior crural septum, until the perforators can be identified in the subcutaneous layer. The bone is now divided into the desired lengths, after which further soft tissue dissection is easier. The soleus muscle is separated from the fibula, leaving a thin strip of muscle (about 1.0 cm) attached to the bone. The flexor hallucis longus mus-
308
cle is separated, and then the peroneal vessels are ligated and cut at the distal end of the flap. The final steps of the dissection are similar to the dissection of a bone-only flap.51–53
Radial Forearm
Osteomuscular-Fasciocutaneous Flap
The fasciocutaneous distal radial forearm flap today seems to be one of the most popular flaps for intraoral reconstruction.54 The thin and pliable flap is pedicled on the radial artery and the deep venae commitantes. For venous drainage of the soft tissue flap, subcutaneous veins from the forearm are also sufficient. The radial artery and the accompanying veins lie in a duplicate of the antebrachial fascia. From there small vessels ascend to the overlying skin, and other vessels descend to the brachioradialis muscle. Together with a part of this muscle, a segment of the radius can be taken, thus turning the fasciocutaneous soft tissue into a fasciocutaneous-osteomuscu- lar radial forearm flap.
Harvesting of the composite radial forearm flap has quite a significant donor site morbidity; radius fractures in up to 20% of the cases have been reported. The available bone is very small in width, height, and length. Therefore, the radial forearm bone and soft tissue flap is not a flap of first choice for functional mandible reconstruction.
References
1.Axhausen W. Die Bedeutung der Individualund Artspezifität der Gewebe für die freie Knochenüberpflanzung. Hefte Unfallheikunde. 1962;72:1.
2.Schweiberer L. Experimentelle Untersuchungen von Knochentransplantaten mit unveränderter und denaturierter Knochengrundsubstanz. Hefte Unfallheilk 103. Berlin: Springer; 1970.
3.Bardenheuer B. Über Unterund Oberkieferresektion. Verh Dtsch Ges Chir. 1892;21:123–130.
4.Sykoff V. Zur Frage der Knochenplastik am Unterkiefer. Zentralbl Chir. 1900;27:81.
5.Krause F. Unterkiefer-Plastik. Zentralbl Chir. 1907;34:1045– 1046.
6.Axhausen G. Histologische Untersuchungen über Knochentransplantationen am Menschen. Dtsch Z Chir. 1908;91:388–428.
7.Lexer E. Die Verwendung der freien Knochenplastik nebst Versuchen über Gelenkversteifung und Gelenktransplantation. Arch Klin Chir. 1908;86:939.
8.Rydygier LRV. Zum osteoplastischen Ersatz nach Unterkieferresektion. Zentralbl Chir. 1908;35:1321–1322.
9.Lindemann A. Über die Beseitigung der traumatischen Defekte der Gesichtsknochen. In: Bruhn C, Hrg. Die gegenwärtigen Behandlungswege der Kieferschußverletzungen. Hefte IV–VI. Bergmann Wiesbaden: 1916.
10.Matti H. Über freie Transplantation von Knochenspongiosa.
Langenbecks Arch Clin Chir. 1932;168:236.
11.Converse JM. Early and late treatment of gunshot wounds of the jaw in French battle casualities in North Africa and Italy. J Oral Surg. 1945;3:112–137.
M. Ehrenfeld and C. Hagenmaier
12.Conley JJ. Use of composite flaps containing bone for major repairs in the head and neck. Plast Reconstr Surg. 1972;49:522.
13.Boyne P. Methods of osseous reconstruction of the mandible following surgical resection. J Biomed Mat. 1973;4:195.
14.Taylor GI, Miller G, Ham F. The free vascularized bone graft. A clinical extension of microvascular techniques. Plast Reconstr Surg. 1975;55:553–554.
15.O’Brien B McC. Microvascular Reconstructive Surgery. Edinburgh: Churchill Livingstone; 1977.
16.Taylor GI, Townsend P, Corlett R. Superiority of the deep circumflex iliac vessels as the supply for free groin flaps. Plast Reconstr Surg. 1979;64:745.
17.Quillen CG. Latissimus dorsi myocutaneous flap in head and neck reconstruction. Plast Reconstr Surg. 1979;63:664.
18.Ariyan S. The viability of rib grafts transplanted with the periostal blood supply. Plast Reconstr Surg. 1980;65:140–151.
19.Swartz WM, Banis JC, Newton ED, Ramasastry SS, Jones NF, Acland R. The osteocutaneous scapular flap for mandibular and maxillary reconstruction. Plast Reconstr Surg. 1986;77:530– 545.
20.Axhausen W. Die Quellen der Knochenneubildung nach freier Transplantation. Langenbecks Arch Klin Chir. 1951;279:439– 443.
21.Axhausen W. Die Knochenregeneration—ein zweiphasiges Geschehen. Zentralbl Chir. 1952;77:435–442.
22.Chalmers J. Transplantation immunity in bone homografting. J Bone Joint Surg. 1959;41B:160–179.
23.Williams RG. Comparison of living autogeneous and homogeneous grafts cancellous bone heterotopically placed in rabbits. Anat Rec. 1962;143:93.
24.Heiple KG, Chase SW, Herndon CH. A comparative study of the healing process following different types of bone transplantation. J Bone Joint Surg 1963;45A:1593.
25.Ray RD, Sabet TY. Bone grafts: cellular survival versus induction. J Bone Joint Surg. 1963;45A:337.
26.Burwell RG. Osteogenesis in cancellous bone grafts: considered in terms of cellular changes, basic mechanisms and the perspective of growth control and its possible aberrations. Clin Orthop. 1965;40:35–47.
27.Lentrodt J, Höltje WJ. Tierexperimentelle Untersuchungen zur Revaskularisation autologer Knochentransplantate. In: Schuchardt K, Scheunemann H, eds. Fortschriffe der Kiefer-und Gesichts-Chirurgie, Vol. 20. Stuttgart: Thieme; 1976:17–21.
28.Eitel F, Schweiberer K, Saur K, Dambe LT, Klapp F. Theoretische Grundlagen der Knochentransplantation: Osteogenese und Revaskularisation als Leistung des Wirtslagers. In: Hierholzer G, Zilch H, eds. Transplantatlager und Implantatlager bei verschiedenen Operationsverfahren. Berlin: Springer, 1980.
29.Schweiberer L, Brenneisen R, Dambe LT, Eitel F, Zwank L. Derzeitiger Stand der auto-, heteround homoplastischen Knochentransplantation. In: Cotta H, Martini AK, eds. Implantate und Transplantate in der Plastischen und Weiderherstellungschirurgie. Berlin: Springer; 1981:115–127.
30.Lentrodt J, Fritzemeier CU, Bethmann I. Erfahrungen bei der osteoplastischen Unterkieferrekonstruktion mit autologen freien Knochentransplantaten. In: Kastenbauer E, Wilmes E, Mees K, eds. Das Transplantat in der Plastischen Chirurgie. Rotenburg: Sasse; 1987:59–61.
31.Steinhäuser EW. Unterkieferrekonstruktion durch intraorale
25. Autogenous Bone Grafts in Maxillofacial Reconstruction
Knochentransplantate—deren Einheilung und Beeinflussung durch die Funktion—eine tierexperimentelle Studie. Schweiz Monatsschr Zahnheilk. 1968;78:213.
32.Reuther JF. Druckplattenosteosynthese und freie Knockentransplantation zur Unterkieferrekonstruktion. Berlin: Quintessenz; 1979.
33.Bell WH. Modem Practice in Orthognathic and Reconstructive Surgery. Philadelphia: WB Saunders; 1992.
34.Sailer HF. Transplantation of Lyophilized Cartilage in MaxilloFacial Surgery. Basel: Krager; 1983.
35.Wolford LM. The use of porous block hydroxyapatite. In: Bell WH, ed. Modern Practice in Orthognathic and Reconstructive Surgery. Philadelphia: WB Saunders; 1992:854–871.
36.Hoppenreijs TJM, Nijdam ES, Freihofer HPM. The chin as a donor site in early secondary osteoplasty: a retrospective clinical and radiological evaluation. J Craniomaxillofac Surg. 1992;20:119–124.
37.Sailer HF, Pajarola GF. Plastische Korrekturen an Weichteilen und Knochen. In: Orale Chirurgie. Stuttgart: Thieme; 1996:308–309.
38.Schliephake H. Entnahmetechniken autologer Knochentransplantate. Implantologie 1994;4:317–327.
39.Tessier P. Autogenous bone grafts from the calvarium for facial and cranial application. Clin Plast Surg. 1982;9:531–538.
40.Maves MD, Matt BH. Calvarial bone grafting of facial defects.
Otolaryngol Head Neck Surg. 1986;95:464–470.
41.Frodel JL, Marentette LJ, Quatela VC, Weinstein GS. Calvarial bone graft harvest: techniques, considerations, and morbidity. Arch Otolaryngol Head Neck Surg. 1993;119:17–23.
42.Payr E. Über osteoplastischen Ersatz nach Kieferresektion (Kieferdefekten) durch Rippenstücke mittels gestielter Brustwandlappen oder freier Transplantation. Zentralbl Chir. 1908;35:1065–1070.
43.Klapp R. Über chirurgische Behandlung der Kieferschußbrüche. Z Ärztl Fortbild. 1916;13:225–232.
44.Rehrmann A. Das freie Knochentransplantat zum Unterkieferersatz unter besonderer Berücksichtigung der Kinnrekonstruktion. In: Schuchardt K, Schilli W, eds. Fortschritte der Kieferund Gesichts Chirurgie, vol. 23. Stuttgart: Thieme; 1978:39.
309
45.Riediger D, Ehrenfeld M. Der vaskularisierte Knochenspan, experimentelle Grundlagen und klinische Anwendung. In: Kastenbauer E, Wilmes E, Mees K, eds. Das Transplantat in der Plastischen Chirurgie. Rotenburg: Sasse; 1987:4–9.
46.Esser E, Mrosk T. Langzeitergebnisse nach Unterkieferrekonstruktionen mit avaskulärem Spongiosatransfer und Titangitter. In: Schwenzer N, ed. Fortschritte der Kieferund Gesichts Chirurgie, vol. 39. Stuttgart: Thieme; 1994:90–92.
47.Michel C, Reuther J, Meier J, Eckstein T. Die Differentialindikation mikrochirurgischer und freier autogener Knochentransplantate zur Rekonstruktion des Unterkiefers. In: Schwenzer N, ed. Fortschritte der Kieferund Gesichts Chirurgie, vol. 39. Stuttgart: Thieme; 1994:96–100.
48.Riediger D, Schmelzle R. Modifizierte Anwendung des myokutanen Latissimus dorsi-Lappens zur Defektdeckung im MundKieferGesichtsbereich. Dtsch Z Mund Kiefer Gesichts Chir. 1986;10:364–374.
49.Jack U. Vergleichende Untersuchung zahnärztlicher Implantatsysteme auf ihre Eignung zur Implantation in Rippentransplantate. Thesis. Germany: University of Tübingen; 1994.
50.Hammer B, Prein J. Differentialindikation mikrochirurgischer Knochentransplantate für die Rekonstruktion des Unterkiefers. In: Bootz F, Ehrenfeld M, eds. Aktuelle Ergebnisse des mikrovaskulären Gewebetransfers im Kopf-Hals-Bereich. Stuttgart: Thieme; 1995:149.
51.Strauch B, Yu HL. Atlas of Microvascular Surgery. New York: Thieme; 1993.
52.Riediger D, Ehrenfeld M. Mikrochirurgie. In: Hausamen JE, Machtens E, Reuther J, eds. Kirschnersche allgemeine und spezielle Operationslehre. Mund-, Kieferund Gesichtschirurgie. Heidelberg: Springer; 1995:559–615.
53.Urken ML, Weinberg H, Vickery C, Buchbinder D, Lawson W, Biller HF. The internal oblique-iliac crest free flap in composite defects of the oral cavity involving bone, skin, and mucosa. Laryngoscope. 1991;101:257–270.
54.Soutar DS. The radial forearm flap in intraoral reconstruction. In: Riediger D, Ehrenfeld M, eds. Microsurgical Tissue Transplantation. Chicago: Quintessence; 1989:31–38.