


396 |
|
|
|
|
|
A.-L. Söderholm, D. Hallikainen, and C. Lindqvist |
||||
TABLE 35.1 Summary of successfully treated late complications (7 of 34 reconstructions).10 |
|
|
|
|||||||
|
|
|
|
|
|
|
Interval |
|
|
|
|
|
|
|
|
|
|
from |
|
|
Follow-up |
|
|
Diagnosis |
|
Plate used |
|
|
primary |
|
|
from |
|
Age |
(stage of |
Resection |
at primary |
Radiation |
|
surgery |
|
Current |
diagnosis |
Patient |
(years) |
disease) |
performed |
surgery |
(dose) |
Complications |
(month) |
Treatment |
state |
(months) |
|
|
|
|
|
|
|
|
|
|
|
1 |
77 |
SCC (IV) |
Left hemi |
AO-RPC |
Postoperative |
Plate fracture |
24 |
AO-RPC free bone |
FFD |
67 |
|
|
|
|
|
(66 Gy) |
|
|
(iliac crest) |
|
|
2 |
66 |
SCC (IV) |
Right body and |
AO-ARP |
Postoperative |
Screw loosening |
12 |
ARP free bone (iliac |
FFD |
53 |
|
|
|
ramus |
|
(66 Gy) |
proximally |
|
crest) dental |
|
|
|
|
|
|
|
|
|
|
implants |
|
|
3 |
77 |
SCC (IV) |
Left body and |
AO-ARP |
Postoperative |
Screw loosening |
18 |
TH-ARP |
AWD |
44 |
|
|
|
ramus |
|
(66 Gy) |
proximally |
|
|
|
|
4 |
60 |
SCC (IV) |
Symphysis right |
AO-ARP |
Postoperative |
Tumor |
12 |
AO-RPC salvage |
FFD |
41 |
|
|
|
body |
|
(66 Gy) |
recurrence |
|
operation |
|
|
5 |
79 |
SCC (IV) |
Symphysis |
AO-SRP |
Preoperative |
Screw loosening |
22 |
TH-SRP |
FFD |
30* |
|
|
|
|
|
(64 Gy) |
proximally |
|
|
|
|
6 |
26 |
Angiosarcoma |
Symphysis right |
W-RPC |
Postoperative |
Extraoral plate |
3 |
Sternocleido |
DFD |
23† |
|
|
(grade II) |
body and |
|
(66 Gy) |
exposure |
|
musculocutaneous |
|
|
|
|
|
ramus |
|
|
|
|
flap |
|
|
7 |
45 |
SCC (IV) |
Right hemi |
AO-RPC |
Postoperative |
Intraoral plate |
6 |
Antibiotics wound |
FFD |
17† |
|
|
|
|
|
(66 Gy) |
exposure |
|
care |
|
|
Abbreviations: AO-ARP, classic angular AO plate; AO-RPC, classic AO plate with condylar head; AO-SRP, classic straight AO plate; AWD, alive with disease; D, dead from other reason; DFD, dead from disease; FFD, free from disease; SCC, squamous cell carcinoma; TH-ARP, AO-THORP angular plate; TH-SRP, AO-THORP straight plate; W-RPC, Würzburg plate with condylar head.
*From diagnosis of mandibular metastasis, 50-month follow-up from primary diagnosis of SCC of the tongue. †Primary plate in place after soft tissue closure.
Source: From ref. 10.
TABLE 35.2 Summary of patient records for late major complications (7 of 34 reconstructions) resulting in plate removal.10
|
|
|
|
|
|
|
|
|
|
Follow-up |
|
|
Diagnosis |
|
|
|
|
|
Interval to |
|
from |
|
Age |
(stage of |
Resection |
|
Radiation |
|
removal |
State of |
diagnosis |
|
Patient |
(years) |
disease) |
performed |
Plate |
(dose) |
Complication |
(month) |
patient |
(months) |
|
|
|
|
|
|
|
|
|
|
|
|
8 |
48 |
SCC (IV) |
Symphysis |
AO-SRP |
Postoperative |
Infection, fistulation |
12 |
FFD |
77 |
|
|
|
|
|
|
(66 |
Gy) |
|
|
|
|
9 |
60 |
SCC (IV) |
Symphysis |
AO-ARP |
|
— |
Infection, fistulation |
10 |
FFD |
66 |
10 |
57 |
SCC (II) |
Symphysis |
AO-SRP |
|
— |
Fistulation |
17 |
FFD |
34 |
|
|
|
|
|
|
|
Plate exposure (partial |
|
|
|
|
|
|
|
|
|
|
flap necrosis) |
|
|
|
11 |
69 |
SCC (III) |
Right ramus |
AO-ARP |
Postoperative |
Chronic infection, |
6 |
D |
25 |
|
|
|
|
body |
|
(66 |
Gy) |
osteoradionecrosis? |
|
|
|
12 |
77 |
SCC (IV) |
Left hemi |
AO-RCP |
Postoperative |
Chronic infection, |
4 |
FFD |
23 |
|
|
|
|
|
|
(66 |
Gy) |
fistulation |
|
|
|
13 |
78 |
SCC (IV) |
Right ramus |
AO-ARP |
Postoperative |
Tumor recurrence, plate |
7 |
DFD |
16 |
|
|
|
|
body |
|
(66 |
Gy) |
exposure |
|
|
|
14 |
61 |
SCC (IV) |
Right ramus |
AO-ARP |
Preoperative |
Tumor recurrence, |
2 |
DFD |
6 |
|
|
|
|
body |
|
(40 |
Gy) and |
infection |
|
|
|
|
|
|
|
|
postoperative |
|
|
|
|
|
|
|
|
|
|
(30 |
Gy) |
|
|
|
|
Abbreviations: AO-ARP, classic angular AO plate; AO-RPC, classic AO plate with condylar head; AO-SRP, classic straight AO plate; AWD, alive with disease; D, dead from other reason; DFD, dead from disease; FFD, free from disease; SCC, squamous cell carcinoma; TH-ARP, AO-THORP angular plate; TH-SRP, AO-THORP straight plate.
Source: From ref. 10.





35. Mandibular Body Reconstruction |
|
|
|
|
|
403 |
||
TABLE 35.5 Radiological examination of screw fixation and plate stability in 13 cases of mandibular reconstructions using the |
|
|||||||
AO-THORP system.15 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First signs |
|
|
|
Number of |
Number of |
State of |
Resorption of |
Resorption of |
of screw |
|
|
|
screws |
screws |
screw |
cortical bone |
cortical bone |
loosening |
Follow-up |
Case |
Resection |
(ramus) |
(body) |
fixation |
buccally |
lingually |
(months) |
(months) |
|
|
|
|
|
|
|
|
|
K |
|
3 |
3 |
good |
— |
— |
— |
6 |
L |
|
2 |
2 |
2 screw |
x* |
— |
1 |
4 |
|
|
|
|
fractures |
|
|
|
|
H |
|
3 |
5 |
good |
xx |
— |
— |
16 |
M |
|
3 |
3 |
good |
xx |
xx |
— |
33 |
N |
|
3 |
3 |
good |
xx |
— |
— |
5 |
O |
|
4 |
4 |
good |
xx |
— |
— |
13 |
P |
|
2 |
4 |
good |
xx |
— |
— |
12 |
Q |
|
2 |
3 |
good |
— |
— |
— |
9 |
R |
|
3 |
3 |
good |
x |
x |
— |
31 |
S |
† |
3 |
3 |
1 screw |
xx† |
— |
3 |
9 |
|
|
|
|
loosened |
|
|
|
|
T |
|
2 |
3 |
good |
xx |
— |
— |
9 |
F |
|
3 |
3 |
good |
— |
— |
— |
35 |
V |
|
2 |
2 |
good |
x |
— |
— |
12 |
Total |
|
35 |
41 |
3 screw |
10 cases with |
2 cases with |
|
|
|
|
|
|
failures |
resorption |
resorption |
|
|
*Tumor recurrence at fixation area.
† secondary reconstruction after radiotherapy. x probable resorption; xx slight resorption.



a |
b |
c |
d |
e |
f |
g
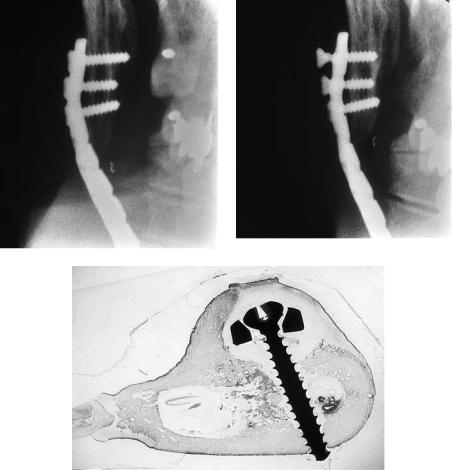
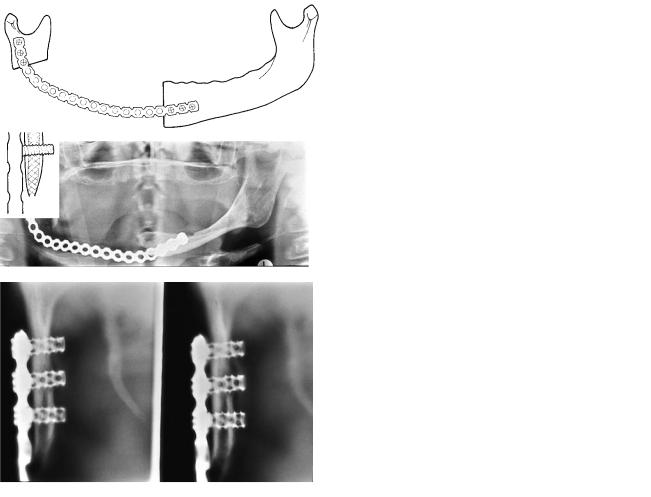
FIGURE 35.11 A large ameloblastoma of the right mandibular angle in a 37-year-old woman was treated by a segmental resection and reconstruction with an AO classic angular plate and multiple nonvascular bone transplants from the iliac crest. (a) A panoramic view of the reconstruction. (b) A diagrammatic representation of
(a). (c) The patient’s mandible after removal of the plate. (d) A diagrammatic representation of (c). (e,f) Rehabilitation of the dentition was performed by dentures. (g) Excellent occlusion, mouth opening, swallowing, mastication, and speech were achieved.