

Upper Limb
page 210
page 211
43 Topographic Anatomy
STUDYAIMS
At the end of your study, you should be able to:
Identifythe bonylandmarks: acromion, coracoid process of scapula, olecranon and head of ulna, medial, and lateral epicondyles, radial styloid process
Identifythe muscle masses of the deltoid, biceps, triceps, brachioradialis, and thenar and hypothenar eminences Identifythe deltopectoral triangle and cubital fossa
Identifythe course of the cephalic, basilic, and median cubital veins
325 / 425
GUIDE
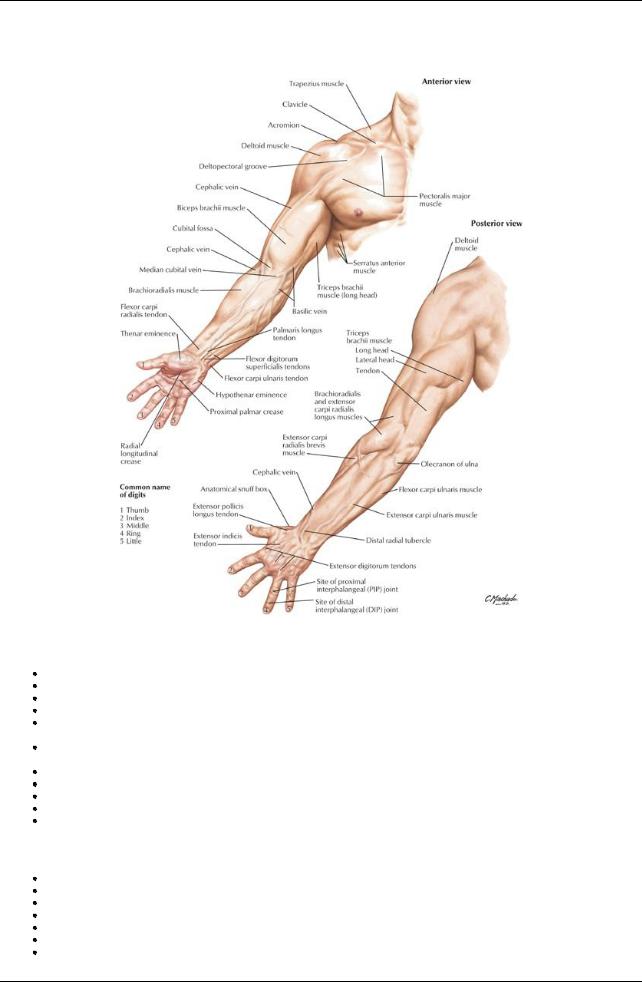
Upper Limb: Topographic Anatomy
[Plate 400, Upper Limb]
Bones
Clavicle: Subcutaneous; palpable throughout its length
Acromion: Easilypalpable, traced mediallyto acromioclavicular joint (see Section 6-2: Upper Limb: Shoulder and Axilla) Coracoid process of scapula: Palpable deep and lateral to the deltopectoral triangle
Head of humerus: Palpable deep to deltoid inferior to lateral edge of acromion when arm is rotated
Elbow: Palpable medial and lateral epicondyles of humerus and visible olecranon process of ulna (see Section 6-4: Upper Limb: Elbow and Forearm)
Head of radius: Palpable as it rotates during pronation and supination on posterolateral aspect of extended elbow, just distal to lateral epicondyle
Ulnar head: Visible on the medial side of the dorsal aspect of the wrist (see Section 6-5: Upper Limb: Wrist and Hand) Radial styloid: Palpable in the anatomical snuff boxon the lateral side of the wrist
Ulnar styloid: just distal to ulnar head with hand supinated Pisiform: hard, round structure on anteromedial aspect of wrist
Tubercles of scaphoid and trapezium: Palpable at proximal end of thenar eminence
Muscles and Tendons
Deltoid muscle: Overlies the shoulder giving it a rounded appearance
Biceps: Bulge on anterior aspect of arm
Biceps brachii tendon: Palpable in cubital fossa, lateral to midline with arm flexed
Flexor tendons: Wrist and finger flexors visible distallyon ventral aspect of forearm
Extensor tendons: Wrist and finger flexors visible on the dorsum of the hand
Thenar eminence: Muscles at the base of the thumb (see Section 6-5: Upper Limb: Wrist and Hand)
Hypothenar eminence: Muscles at the base of the little finger (see Section 6-5: Upper Limb: Wrist and Hand)
326 / 425
Arteries and Veins
page 211 page 212
Brachial artery
Pulsations can be palpated deep to medial border of biceps muscle
Used to determine heart rate in children
Radial artery: Pulse can be felt bycompressing arteryagainst distal end of radius
Median cubital vein (see Section 6-4: Upper Limb: Elbowand Forearm)
Traverses the cubital fossa connecting cephalic to basilic veins
Often used for venipuncture
Cephalic vein ascends along lateral forearm and arm (see Section 6-6: Upper Limb: Neurovasculature)
Basilic vein ascends along medial forearm and distal arm (see Section 6-6: Upper Limb: Neurovasculature)
Dorsal venous network seen on the dorsum of the hand
Nerves
Ulnar nerve can be felt under the medial epicondyle
327 / 425
FACTS & HINTS
HIGH-YIELD FACTS
Anatomic Points
Functional Overview
The upper limb is highlymobile and characterized byits abilityto perform a wide range of controlled movements to manipulate the surrounding environment. It is suspended from the trunk at the shoulder, and its stabilityhas been sacrificed to gain mobility. Clinicallythe limb is divided into four regions: pectoral girdle, arm, forearm and hand.
Upper Limb Development
The upper limb buds from the embryonic trunk and rotates 90 degrees laterally, such that in the anatomic position, the ventral structures face anteriorlyand the dorsal structures posteriorly. This contrasts with the medial rotation of the lower limb. Thus, the upper and lower limbs are 180 degrees out of phase. Flexors of all joints in the upper limb are anterior, and extensors are posterior.
Clinical Points
Winged Scapula
Normallythe scapula is held closelyagainst the posterior thoracic wall. Damage to the long thoracic nerve to serratus anterior (which courses superficiallyover the muscle) causes "winging" of the scapula as its medial border lifts awayfrom the thoraxwhen the arm is raised. This is accentuated when the individual leans on the hand or pushes the upper limb against a wall. Most importantly, the arm cannot be abducted above the horizontal plane because glenoid cavitycannot be rotated upward without the action of the serratus anterior.
328 / 425

44 Shoulder and Axilla
STUDYAIMS
At the end of your study, you should be able to:
Identifythe different parts and surface markings of the clavicle and scapula
Describe the sternoclavicular, acromioclavicular, and glenohumeral joints, their movements, and supporting ligaments Understand the organization of the scapular muscles
Know the origins, insertions, and actions of the intrinsic scapular muscles Identifythe boundaries of the axilla and describe its contents
Describe the organization of the deep fascia
329 / 425