

The Physics of Coronory Blood Flow - M. Zamir
.pdf1.4 Coronary Arteries |
7 |
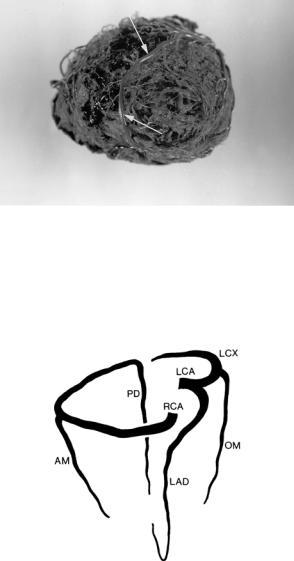
Fig. 1.3.2. Origin of the left main and right coronary arteries (LCA, RCA) and two additional branches (black arrows) as they arise from the aorta. From a cast of a human coronary network [216].
1.4 Coronary Arteries
As the left main and right coronary arteries leave the aorta they circle the heart in the manner of a crown, hence the name “coronary” arteries. The attributes “left” and “right” relate to the fact that the left coronary artery circles the left side of the heart while the right coronary artery circles the right side, though the situation is not accurately so. Furthermore, while the term “coronary” was first applied to the two main supplying arteries, it is now used to include all branches and sub-branches of these vessels as well as the capillary and venous vasculature, which in total comprise the “coronary circulation”. Thus, in general terms, the word “coronary” has come to mean any element of blood supply to the heart for its own metabolic needs.
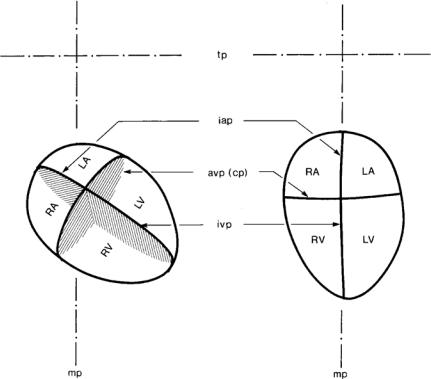
The left main and right coronary arteries encircle the heart along the atrioventricular groove, in the atrioventricular sulcus, formed between the ventricular and atrial chambers of the heart [133]. Their points of origin from the aorta are somewhat above this groove, thus each begins its course by proceeding down towards the groove. In this description, and in what follows, the heart is imagined in an upright position, with the atria at the top and ventricles at the bottom (Fig.1.4.1). If the heart is positioned in this way within the body, its left and right sides coincide approximately with the left and right sides of the body. Wide variations in the layout of the coronary arteries from one heart to another make only approximate descriptions possible. Furthermore, it is important to di erentiate between exact anatomical mapping of
81 Static Design Issues
Fig. 1.4.1. (left) Approximate anatomical orientation of the heart (in a front view) in relation to the median and transverse planes of the body (mp, tp). (right) A “theoretical” upright position in which the heart is turned so that its atrioventricular plane (avp) is approximately parallel to the transverse plane of the body, and the interatrial and interventricular planes (iap, ivp) are approximately parallel to the median plane of the body. This position is convenient for discussion since here the left and right sides of the heart coincide approximately with the left and the right sides of the body. The main coronary arteries circle the heart in the atrioventricular plane, which is hence also known as the coronary plane (cp). From [228].
the coronary arteries in a given heart, and approximate functional layout of these vessels in every heart. The first may be important for the purpose of clinical intervention and treatment in a particular heart. The second relates to fluid dynamic design and function of the coronary network in general, and it is the main focus in this book.
As the left main coronary artery reaches the atrioventricular groove, it bifurcates into two major branches [133]. One, known as the left anterior descending artery, heads down along the interventricular groove, which overlies a thick muscular wall between the left and right ventricular chambers (Fig.1.4.2). This wall, known as the interventricular septum, actually func-
1.4 Coronary Arteries |
9 |
APEX
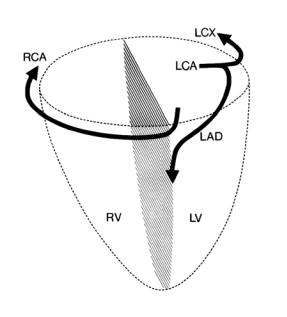
Fig. 1.4.2. The way in which the main coronary arteries circle the heart (in a front view), in relation to the coronary plane (dashed circle) and the interventricular plane (hatched plane). The right coronary artery (RCA) circles the right side of the heart while the left circumflex artery (LCX), which is a main branch of the left main coronary artery (LCA), circles the left side of the heart. The left anterior descending artery (LAD), which is the other main branch of the left main coronary artery, descends along the edge of the interventricular wall toward the apex of the heart. From [216].
tions as part of the left ventricle, hence blood supply to it is particularly important. The other branch, known as the left circumflex artery, turns to circle the left side of the heart along the atrioventricular groove. As it does so it gives rise to a number of small branches which head up to serve the right atrial region, and larger branches which head down to serve the lateral and posterior walls of the left ventricle (Fig.1.4.3).
As the right coronary artery reaches the atrioventricular groove, it turns to circle the right side of the heart, coursing along the groove and giving rise to branches heading up to serve the right atrial region and down to serve the anterior and posterior walls of the right ventricle (Fig.1.4.3). In approximately 90% of human hearts, as the right coronary artery reaches the atrioventricular groove at the back of the heart, it gives rise to an important branch known as the posterior descending artery [133]. This branch runs down along this groove to serve the posterior interventricular septum, in the same way that the anterior descending artery serves the anterior interventricular septum. Indeed

10 1 Static Design Issues
Fig. 1.4.3. Cast of the coronary network of a human heart in which the left main coronary artery and its branches are seen in light grey and the right coronary artery and its branches are seen in black. The heart is here viewed from the back. The left circumflex artery (lcx) is seen circling the left side of the heart and giving rise to a number of large branches (lvlcx) to serve the left ventricular wall. The right coronary artery is seen to do the same on the right side of the heart, giving rise first to some small branches that serve the right ventricular wall, but then a large branch known as the posterior descending artery to serve the interventricular wall from the back. From [228].
1.4 Coronary Arteries |
11 |
Fig. 1.4.4. The left anterior descending artery, which descends along the front edge of the interventricular wall (Fig.1.4.2), is seen here wrapping itself around the apex of the heart (see also Fig.1.4.5). It then begins to ascend along the back edge of the interventricular wall, as if to meet the posterior descending artery which is descending toward it along that edge. From [228].
Fig. 1.4.5. The main “skeleton” of the coronary arterial network and the way in which it serves di erent regions of the heart. The right coronary artery (RCA) and the left circumflex artery (LCX) circle the heart as a belt or a “crown”, sending branches up to serve the atria and down to serve the ventricles. Of the latter the most important are the left anterior descending artery (LAD) and the posterior descending artery (PD) which together circle and serve the interventricular wall. Two other main branches, the acute marginal (AM) and obtuse marginal (OM), serve the right and left arterial walls, respectively. This skeleton is supplemented by many other branches of a wide range of sizes and in a highly variable pattern (see Fig.1.4.3).
12 1 Static Design Issues
both arteries head towards each other as they move towards the “apex”, the pointed bottom of the heart. In most cases the anterior descending artery then wraps around the apex (Fig.1.4.4) and the two vessels stop short of meeting thereafter (Fig. 1.4.5). In 70% of human hearts the right coronary artery continues to circle the heart, after giving rise to the posterior descending artery, to serve some of the posterior wall of the left ventricle [133].
1.5 Left/Right Dominance
With the heart in an upright position, the right coronary and left circumflex arteries circle the heart in a horizontal (coronary) plane, and in opposite directions (Fig. 1.4.2). As they reach the back of the heart, the two arteries move toward each other and terminate short of actually meeting (Fig. 1.5.1). The point at which this occurs is a measure of the extent to which the right coronary artery supplies the left side of the heart, which is an important functional aspect of the coronary network usually referred to as left/right dominance [133]. An important anatomical landmark in this subject is the “crux”, the point at which the horizontal atrioventricular groove crosses the vertical interventricular groove at the back of the heart (Fig. 1.5.1). At approximately this point the posterior descending artery arises and begins its descent along the interventricular groove to serve the interventricular wall. Whether this artery arises from the right main coronary artery or from the left circumflex artery depends on which of the two arteries reaches the crux.
In only 10% or so of human hearts, the left circumflex artery reaches the crux and gives rise to the posterior descending artery [133]. Such cases are known as “left dominant” since, functionally, blood supply to the left ventricle then depends entirely on the left coronary artery. In approximately 20% of human hearts, known as “balanced” cases [133], the right coronary artery reaches the crux, gives rise to the posterior descending artery and terminates at that point. In the remaining 70% of cases, known as “right dominant”, the right coronary artery continues beyond the crux to serve part of the posterior wall of the left ventricle.
Thus, in the large majority of human hearts, blood supply to the left ventricle is shared by the left and right main coronary arteries, not necessarily equally but in parallel, thus providing two sources of supply instead of one. While this has a clear design advantage, the relative extent to which the two arteries share their service to the left ventricle is highly variable. At one extreme the right coronary artery may not serve the left ventricle at all, thus leaving that ventricle, including the interventricular wall, to depend entirely on the left circumflex artery. At the other extreme the right coronary artery may supply the interventricular wall as well as the entire back wall of the left ventricle (Fig. 1.5.2). Since this wide range of variability represents the variable extent to which blood supply to the left ventricle may depend on one or two main lines of supply, the degree of left/right dominance in a given heart

1.6 Branching Structure |
13 |
Fig. 1.5.1. As the right coronary artery (RCA) and the left circumflex artery (LCX) reach the back of the heart they move toward each other. Only one of them reaches the “crux” and gives rise to the posterior descending artery (PD). The numbers identify individual walls of the two ventricles: (1) interventricular septum, (2,3) lateral and posterior walls of the left ventricle, respectively, (4,5) posterior and anterior walls of the right ventricle, respectively. It is seen that the interventricular septum, which separates the two ventricles, is in fact an important part of the left ventricle. From [216].
may be regarded as an “anatomical risk factor”. While an exact numerical measure of that risk factor based on a measure of left/right dominance is not easy to calculate, the connection between the two measures is clear.
More generally, the concept of left/right dominance highlights the wide range of variability in the detailed layout of the coronary arteries and their branches, and hence the need to refer to these vessels by function rather than name. A vessel referred to by the same name in di erent hearts rarely serves precisely the same fluid dynamic function in every heart. It is as important to assess the role of a given artery in the general scheme of blood supply to a given heart as it is to assess the degree of stenosis in that vessel.

14 1 Static Design Issues
Fig. 1.5.2. Casts of the arterial networks of human hearts in which the distribution of the left main coronary artery is seen in red (a,c,f) or yellow (b,d,e) and the distribution of the right coronary arteries is seen in blue (a,b,c,d,f) or green (e). The hearts, in all cases, are in an upright posterior view. The figure illustrates the range of variability in the way in which the two arteries share the responsibility of cardiac blood supply. At one extreme (a), known as “left-dominant”, the left coronary artery gives rise to the posterior descending artery and therefore blood supply to the left ventricle depends on vasculature arising entirely from the left coronary artery. In a “balanced” case (b), the right coronary artery gives rise to the posterior descending artery and thereby contribute to blood supply to the interventricular wall, which is an important part of the left ventricle. In “right-dominant” cases, the right coronary artery continues beyond the crux to supply part or all the posterior wall of the left ventricle (c,d,e,f), thereby taking a greater share of the supply to that ventricle. From [216]. (See color insert.)
1.6 Branching Structure
The question of whether the arterial system of the heart has the structure of an “open tree” or an “interconnected mesh” is one of whether blood supply to any region of the heart can reach it via more than one path. In an open tree structure a main supplying artery, such as the left main or right coronary artery, divides into (usually two) branches, then each of these branches in turn divides into further branches, and so on. There are no “collateral” connections between branches. Flow from the main supplying artery to any peripheral branch can reach it only by progressing along the strict hierarchical structure of the tree, from parent to branch at each junction. That is, the flow can only reach its destination via one distinct path (Fig. 1.6.1). In an interconnected

1.6 Branching Structure |
15 |
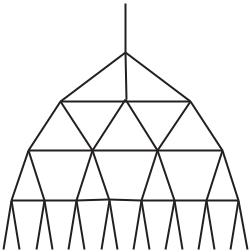
Fig. 1.6.1. In an open tree structure, shown schematically here, flow from the main supplying artery (top) must proceed along the strict branching hierarchy of the tree, that is from parent to branches at each junction. Each destination (bottom) can be reached via only one distinct path. Symmetry and uniformity are not necessary but are used here to emphasize these hierarchical features. Arterial trees are generally nonsymmetrical and highly nonuniform, but their underlying architecture is most often that of an open tree structure.
mesh structure, or in an open tree structure with an overlay of collateral connections, by contrast, there may be several paths to any given destination (Figs. 1.6.2, 3).
This issue is of particular functional and clinical importance. In the presence of multiple paths blood supply can bypass an occluded vessel segment and reach its destination via a di erent path, an important consideration since occluded or obstructed blood vessels are the cause of most heart failures [3, 17, 209, 83, 81, 14]. But the subject is highly controversial, for several reasons. First, because the presence of collateral vessels in the vascular system of the heart is highly variable in di erent species. Second, because the presence of collateral vessels in the human heart is found to be highly variable not only from heart to heart but also in the same heart at di erent times. Thus, the way in which collateral vasculature fits in the hemodynamic design of the coronary circulation in general, and in that of the human heart in particular, is not fully established.
Remarkably, as early as the seventeenth century it was observed that “The vessels which carry blood to the heart .. come together again and here and there communicate by anastomosis” [126]. Two centuries later: “The human heart is potentially able to develop collaterals where they are needed” [93]. And more recently, by various casting and injection techniques, investigators
16 1 Static Design Issues
Fig. 1.6.2. In an interconnected mesh structure flow from the main supplying artery (top) can reach its destinations (bottom) via di erent routes. Early studies of dog coronary vasculature indicated that its underlying architecture has this interconnected structure. Subsequent work on the human heart, on the other hand, showed repeatedly that the underlying architecture of its vasculature is that of an open tree structure. Interconnected mesh structures in the vascular system occur mostly at the capillary level. At higher levels of the system they are rare because an open tree structure is, fluid dynamically, more e cient than an interconnected mesh.
demonstrated clearly the existence of such collateral vasculature, abundant in the dog heart, rarely or scarcely found in the pig, and variable in the human heart [185, 173, 27, 15, 69, 16, 74, 95]. While di erences between species suggest that collateral vasculature may be part of the hemodynamic design of the coronary circulation in some species, the matter is far from settled. Much of the focus has been on the situation in the human heart.
An extensive study by Baroldi and Scomazzoni [16] sums up much of our current understanding of collateral vasculature in the human heart and resolves much of the controversy relating to variability. By a systematic survey of human hearts the authors found that both the number and size of collateral vessels were strongly linked to the presence of an ischemic history or conditions within the heart. Very fine collateral vasculature may be found sporadically here and there when ischemic conditions are absent, but in the presence of such conditions collateral vasculature becomes more significant in size and clearer in its mission. The results clearly established the phenomenon of collateral vasculature as a compensatory mechanism in coronary heart disease [15, 14], and this is how the matter rests.
But the question of the e ectiveness of this mechanism is far from settled, and controversy continues to surround this aspect of the phenomenon.