


CHAPTER FOUR
Evaluation of Size, Function, and Hemodynamics
The ability to identify cardiac chambers and valves via M-mode ultrasound was a major breakthrough in the field of cardiology. Structure and function could be assessed noninvasively. The advent of twodimensional echocardiography permitted easier diagnosis of disease as the relationships between structures were seen. Two-dimensional and M-mode ultrasound provide data regarding size and structure as well as some hemodynamic information, but Doppler ultrasound provides so much information about intracardiac pressures, stroke volumes, regurgitant fractions, shunt ratios, and systolic and diastolic function, that most invasive cardiac tests are no longer necessary. There are many general reference articles discussing the principles of echocardiography and its interpretation (1–13). This chapter discusses the assessment of cardiac structure, size, function, and hemodynamics obtained from M-mode, two-dimensional and Doppler studies.
Measurement and Assessment of Two-Dimensional Images
Subjective Impression of Size
Even before quantitative measurements are made from M-mode or two-dimensional images, impressions of size and function can be obtained from two-dimensional images. It is possible, in most cases, to finish a two-dimensional exam without having made any quantitative measurements and have a very good impression of size and function. What follows are guidelines for subjectively interpreting two-dimensional images.
Right Parasternal Long-Axis Left Ventricular Outflow View
When a clear right ventricular wall is seen, its thickness is usually about 1/3 to 1/2 the thickness of the left ventricular free wall. An increase in right ventricular wall thickness suggests the presence of right ventricular hypertrophy (Figure 4.1). The interventricular septum is typically slightly thicker than the left ventricular free wall in dogs and cats, but can be much thicker than the free wall in horses especially foals (Figure 4.2) (14–19). In the presence of right ventricular hypertrophy, the interventricular septum may also be hypertrophied so compare the right ventricular wall to the left ventricular free wall. When quantitative measurements reveal a thin left ventricular wall, then the relationship of right ventricular wall thickness to left ventricular wall thickness should be reevaluated.
Left Ventricular Outflow View
Assessment (Dogs)
There is no curving of the IVS.
IVS and LVW are similar in size.
IVS does not extend into LVOT.
RV wall is about 1/2 thickness of LVW.

RV chamber size is about 1/3 of LV chamber size.
LA and AO are similar in size.
MV excursion almost to IVS.
There are no valvular lesions.
Figure 4.1 Right ventricular wall thickness (arrows) should be approximately 1/3 the thickness of left ventricular wall thickness in normal animals. The interventricular septum is typically about the same thickness as the left ventricular wall in dogs and cats. RV = right ventricle, IVS = interventricular septum, LV = left ventricle, AO = aorta, MV = mitral valve, LA = left atrium, LVW = left ventricular wall.
Figure 4.2 The normal interventricular septum in horses is usually much thicker than the left ventricular wall. RV = right ventricle, IVS = interventricular septum, LV = left ventricle, AO = aorta, MV = mitral valve, LA = left atrium, LVW = left ventricular wall.

The interventricular septum should be straight and not curve toward the right or left ventricle during diastole. Displacement toward the right side of the heart indicates left ventricular volume overload (Figure 4.3) and displacement toward the left side of the heart tends to indicate right ventricular volume or pressure overload, or in some cases may be a manifestation of left ventricular hypertrophy (Figure 4.4). Many normal cats have a slight upward curve of the interventricular septum (Figure 4.5). Biventricular dilation often keeps the pressure relationship between both ventricles the same, and bowing of the septum will not be present. The relationship of right ventricular size to left ventricular size in a normal heart should be approximately 1 to 3 (Figures 4.1, 4.6).
Left Ventricular Outflow View
Assessment (Cats)
Slight bowing of the IVS is possible.
IVS and LVW are similar in size.
IVS extends slightly into LVOT.
RV wall is about 1/2 thickness of LVW.
RV chamber size is about 1/3 of LV chamber size.
LA is up to 1.7 times size of the AO.
MV excursion is almost to IVS.
There are no valvular lesions.
Figure 4.3 Bowing of the interventricular septum toward the right ventricle indicates left ventricular volume overload (arrow). This image also shows a mildly dilated left atrium (double-headed arrow), which should be approximately the same size as the aorta. RV = right ventricle, LV = left ventricle, VS = ventricular septum, LVW = left ventricular wall, AO = aorta, LA = left atrium, PA = pulmonary artery.
Figure 4.4 (A) Right ventricular volume overload in this horse displaces the interventricular septum downward toward the left ventricle. (B) Hypertrophy of the septum will cause it to extend further into the left ventricular chamber and outflow tract than normal (arrow) as seen in this dog with subaortic stenosis. RV = right ventricle, LV = left ventricle, AO = aorta, LA = left atrium.
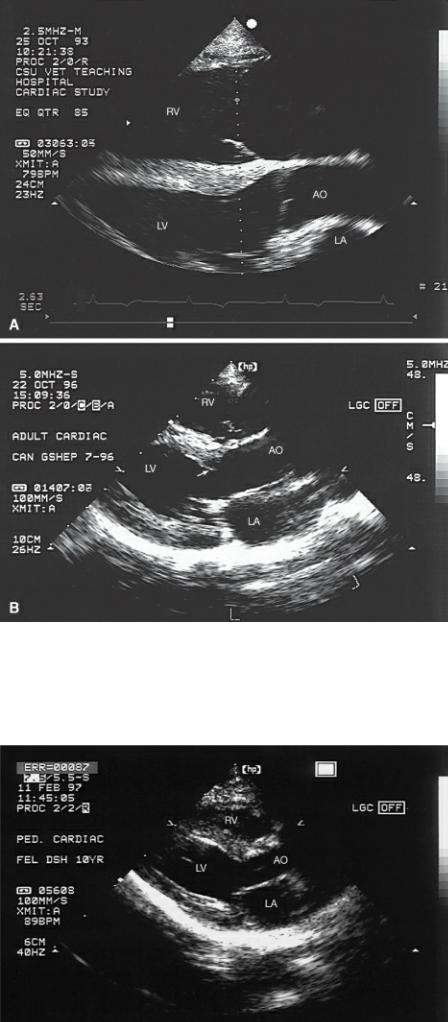
Figure 4.5 The base of the interventricular septum in normal cats tends to protrude into the left ventricular outflow tract slightly. RV = right ventricle, LV = left ventricle, LA = left atrium, AO = aorta.

Figure 4.6 An approximate ratio of right ventricular chamber to left ventricular chamber that exceeds 1:3 indicates right ventricular volume overload as seen in this dog with pulmonic stenosis and insufficiency. The right ventricular wall is also hypertrophied. RV = right ventricle, RA = right atrium, LV = left ventricle, AO = aorta, LA = left atrium.
The interventricular septum in all animals but cats should also not extend into the left ventricular outflow tract. The width of the outflow tract should be about the same as the width of the aortic root (Figure 4.1). The interventricular septum in many healthy cats tends to extend slightly into the outflow tract making the outflow tract width about 3/4 the size of the aortic root (Figure 4.7).
Figure 4.7 The left atrium (large arrows) in normal cats can be up to 1.6 times larger than the aorta (small arrows). RV = right ventricle, LV = left ventricle, AO = aorta, LA = left atrium.
The relationship of wall thicknesses and chamber sizes are different in neonates. Right ventricular wall thickness is as great or greater than left ventricular wall thickness in all neonates (14,15). Right ventricular chamber size is also larger in neonates, and the volume may remain large for several weeks (14,15). Assessment of cardiac size in neonates is often a challenge, and unless there is clear pathology, re-evaluation of the heart may be necessary after the animal is 3 to 6 months old.
Although left atrial size may be slightly larger than aortic root size, visually the left atrial to aortic

ratio should appear to be about 1 to 1 in the dog. Cats tend to have a larger atrium with respect to the aorta than dogs, and the visual ratio of left atrium to aorta may be 1.6 to 1.0 in healthy cats (Figures 4.5, 4.7) (18,19). The ratio of left atrium to aorta in all animals can be deceiving if the aortic root itself is small or large, and so this ratio is only a rough assessment of atrial size.
Enlargement of the left atrium may be seen in planes other than the long axis. For this reason, measurements of left atrial size may be more accurate when taken from several two-dimensional imaging planes, and any one echocardiographic image should not be used solely to assess cardiac size (20,21).
Left atrial size decreases within hours after birth as the ductus and foramen close resulting in decreased atrial volume so echocardiographic exams even at several weeks of age should show the same left atrial to aortic root ratio as that seen in mature animals (15). The newborn foal has a smaller LA/AO ratio than humans, cats, or dogs (14,15). This suggests smaller left atrial size at birth and less atrial enlargement secondary to the ductus arteriosus.
The tip of the septal mitral valve leaflet should almost touch the ventricular septum during diastole. The leaflet should extend straight out from the annulus. There should be no convex or concave shape to the leaflet at end diastole (Figure 4.8). An abnormal shape at end diastole could indicate decreased left ventricular ejection fraction, severe aortic insufficiency, or mitral stenosis. The valve itself should appear to be the same thickness throughout its length from the base of the leaflet, where it attaches near the aortic root, to its tip. This is best assessed during diastole when the valve is wide open and not during systole when the leaflet edges are touching each other and may appear thick. Do not mistake chordae tendinae for lesions as they extend from the leaflets especially when the valve is closed (Figure 4.9).
Left Ventricular Outflow View
Assessment (Horses)
There is no bowing of the IVS.
IVS is thicker than LVW.
RV wall is about 1/2 thickness of LVW.
RV chamber size is about 1/2 of LV chamber size.
LA is smaller or the same size as AO.
MV excursion is almost to IVS.
There are no valvular lesions.
Spontaneous contrast may be seen.
Figure 4.8 The anterior mitral valve leaflet should extend straight out to the ventricular septum during diastole with no curving. RV = right ventricle, LV = left ventricle, AO = aorta, LA = left atrium, MV = mitral valve.
Figure 4.9 Chordae tendinae can be mistaken for lesions when the mitral valves are closed (arrow) on both (A) left ventricular outflow views and (B) four-chamber views. RV = right ventricle, LV = left ventricle, AO = aorta, LA = left atrium, RA = right atrium.
Spontaneous echo contrast is seen within the right ventricular chamber and sometimes the left

ventricle of horses in all planes. This smoke-like swirling of visible blood is reported in approximately 50% of horses examined echocardiographically, and although considered to be a normal finding, it is also seen in horses with exercise-induced pulmonary hemorrhage (22). Spontaneous echo contrast is especially prevalent in racehorses with a reported 93% occurrence. Increasing age, male gender, and pregnancy increases the occurrence of contrast. High heart rates also increase the amount of contrast seen (22).
The smoke-like echoes of circulating blood have also been reported in experimental healthy sedated dogs (23). It is seen more readily with high frequency transducers than low frequency transducers in the same animal because of increased lateral and longitudinal resolution (23). It has not been reported in clinically healthy unsedated or unanesthetized dogs.
Right Parasternal Long-Axis Four-Chamber View
Right ventricular chamber size appears slightly larger in right parasternal long-axis four-chamber views than in the right parasternal inflow outflow long-axis plane, but the 1-to-3 relationship with the left ventricle should still predominate. The interventricular septum should extend straight to the apex of the heart, parallel to the left ventricular wall with only a slight deviation to the right at the base of the septum near the mitral valve annulus (Figure 4.10).
Four-Chamber View
Assessment (All Animals)
There is no curving of the IAS or IVS.
There are no valvular lesions.
Figure 4.10 Other than a slight deviation away from the AV junction, the interventricular septum should be straight with no bowing to the right or left on four-chamber views as seen in this (A) horse and this (B) dog. The interatrial septum should also be straight with no deviation to the right or left. (C) Bowing of the interventricular and interatrial septums to the right side of the heart is indicative of left ventricular and left atrial volume overload. RV = right ventricle, RA = right atrium, LV = left ventricle, LA = left atrium, IAS = interatrial septum.

The atrial septum should also be straight with no curvature to the right or left side of the heart. There is often a thinner area midway along the atrial septum that at times looks like an opening (Figure 4.11). This thin area of tissue is the fossa ovalis, the membrane that closed the foramen ovale. The right atrium may appear somewhat smaller than the left atrium in this view. The tricuspid annulus is slightly closer to the apex of the heart than the mitral annulus but not by more than a millimeter or

two. Right ventricular to left ventricular free wall thickness ratios are often easier to visualize in this imaging plane and should be about .5-to-1.0.
Figure 4.11 A thinner area of echogenicity midway along the atrial septum represents the membrane that closed the foramen ovale (arrow). RA = right atrium, LV = left ventricle, LA = left atrium.
This four-chamber view of the heart is excellent for examination of the atrioventricular valves. Valve thickness should remain the same from the base of the leaflet to its tip. The closed AV valve should have a concave curve toward the ventricular chamber as they extend from the annulus (Figure 4.10).
Right Parasternal Transverse Left Ventricle
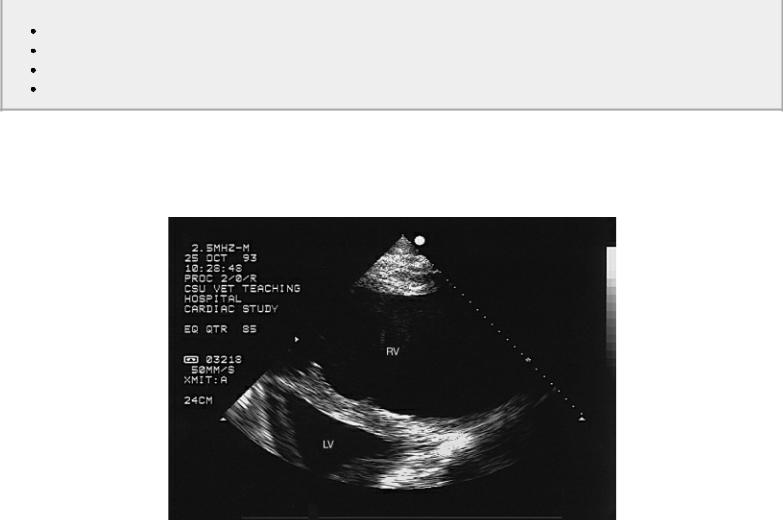
A good transverse view of the left ventricular chamber at the level of the papillary muscles should be round and symmetrical. The left ventricular lumen should have a mushroom shape. The papillary muscles should be similar in size, and the septum should not be flattened. Right ventricular pressure or volume overload often flatten the septum creating a triangular-shaped left ventricular chamber (Figure 4.12). The septum and free wall, excluding the papillary muscles, should be similar in size in small animals, while the septum is usually thicker than the free wall in horses. The right ventricular chamber should be crescent-shaped in all animals. Transverse sections of papillary muscles and trabecular irregularities on the right ventricular side of the septum are common and normal in this view (Figures 4.13, 4.14).
Transverse Left Ventricle
Assessment (Cats and Dogs)
Uniform shortening
Circular outer shape
Mushroom LV internal shape
Symmetrical papillary muscles
Transverse Left Ventricle
Assessment (Horses)
Uniform shortening
Circular outer shape
Triangular LV internal shape
Symmetrical papillary muscles
Figure 4.12 This horse’s interventricular septum on the transverse plane is flattened and pushed toward the left ventricle indicative of elevated right ventricular diastolic pressure and volume overload. RV = right ventricle, LV = left ventricle.
Figure 4.13 Both of these images show normal irregularities on the right ventricular side of the septum (arrows). RV = right ventricle, VS = ventricular septum, LV = left ventricle, LVW = left ventricular wall.

Figure 4.14 Right ventricular papillary muscles are often seen in cross section on transverse images of the left ventricle (arrow). RV = right ventricle, LV = left ventricle.
Right Parasternal Transverse Heart Base
Diameters of the aorta and pulmonary artery at the level of their valves should be similar on right parasternal transverse images of the heart base (Figure 4.15). Enlargement of the pulmonary artery

may be seen with poststenotic dilation or volume overload. Pulmonary valve cusps often have a slight upward curvature to them. There should be no change in diameter of the pulmonary artery from the level of the pulmonary valve to the bifurcation. Diameters of the aorta and left atrium in the dog should also be fairly close to the same size in this plane (Figure 4.16). The cat has a larger left atrium compared to the aorta.
Transverse Heart Base
Assessment (Dogs)
Aorta and pulmonary artery are similar in size.
Left atrium and aorta are similar in size.
Transverse Heart Base
Assessment (Cats)
Aorta and pulmonary artery are similar in size.
Left atrium is larger than aorta.
Transverse Heart Base
Assessment (Horses)
Aorta and pulmonary artery similar in size
Aorta clover shaped
Left atrium smaller or the same size as aorta
Figure 4.15 The pulmonary artery and aorta should have very similar dimensions on transverse images of the heart base. Here the pulmonary artery is very dilated, and even the left main pulmonary artery is easily visualized. RV = right ventricle, RA = right atrium, AO = aorta, PA = pulmonary artery, RMPA = right main pulmonary artery, LMPA = left main pulmonary artery.
Figure 4.16 Diameters of the aorta and left atrium should be similar in size on transverse views. This dog with mitral insufficiency has a severely dilated left atrium. RV = right ventricle, AO = aorta, LA = left atrium, LAA = left auricular appendage.

Quantitative Measurement of Size
Two-dimensional measurements of size have been reported for the cat and dog (20,21). Instructions for measuring the various cardiac dimensions from two-dimensional images are described here, and the reference values can be found in the appendices. The use of tissue harmonic imaging, although it enhances images, does lead to small increases in measurements of wall and septal thicknesses and small decreases in chamber sizes (24). These differences are probably minimal but should be kept in mind. Reference ranges in this book are derived from fundamental imaging. Measurements from twodimensional images are a very viable option when M-mode images are not of good diagnostic quality or the M-mode cursor cannot be aligned properly.
Measurements of cardiac size obtained from two-dimensional images involve freezing the image at end diastole and at end systole. End diastole is identified as the largest left ventricular dimension just before or as the mitral valve closes. End systolic frames are identified as the smallest ventricular chamber size just before the mitral valve opens. Measurements of chamber size are obtained from the endocardial surface of the ventricular septum to the endocardial surface of the left ventricular wall. This is called the trailing edge to leading edge method. Left ventricular wall measurements are taken from the top of the wall, including the endocardial surface to the top of the pericardial sac. Septal measurements however are made from the trailing edge of the right side of the septum to the trailing edge of the left ventricular side of the septum. Therefore, the line defining the top of the interventricular septum is not included in the septal thickness measurement. Measuring planes are similar for dogs and cats. The only exception involves measurement of the left ventricular wall, septum, and chamber from the right parasternal long-axis view in the dog. The measurements in dogs were derived from images that do not have a well-defined aorta while the measurements in cats were obtained from standard left ventricular inflow outflow imaging planes (19–21).
Left Ventricular Chamber, Wall, and Septum
Measurements of the minor dimension through the left ventricular chamber are made from a right parasternal long-axis view that includes part of the left ventricular outflow tract and aortic valve, the left atrium, and mitral valve (Figure 4.17). A line perpendicular to the septum and the wall just beyond the tips of the mitral valves at the largest left ventricular dimension when they are wide open
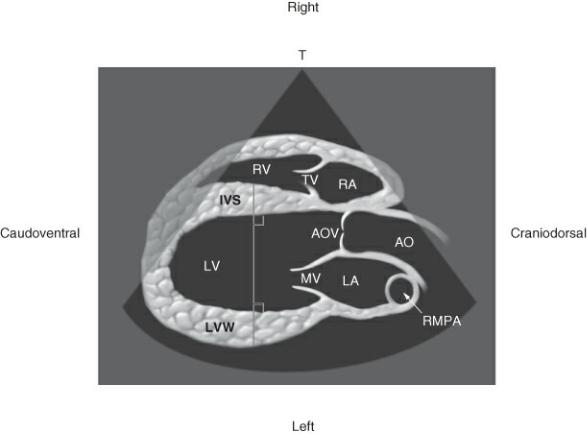
is used to identify the measurement location for this left ventricular diameter. Advance the image until the largest and smallest chamber sizes corresponding to diastolic and systolic dimensions respectively are identified.
Figure 4.17 Measure the left ventricular chamber, septum, and wall from right parasternal long-axis left ventricular outflow views at the largest and smallest left ventricular chamber sizes. A line is drawn perpendicular to the wall and septum. This line is used as the reference points for measurement during both diastole and systole. RV = right ventricle, TV = tricuspid valve, RA = right atrium, IVS = interventricular septum, AOV = aortic valve, AO = aorta, MV = mitral valve, LA = left atrium, LVW = left ventricular wall, RMPA = right main pulmonary artery.
The minor chamber size may also be measured from the right parasternal short-axis view of the heart at the level of the chordae tendinae (Figure 4.18). A line connecting the septum and wall, dividing the ventricle into equal and symmetrical mirror image halves is used to identify measuring points. The line should be perpendicular to a line connecting the chordae on each side of the image.
Figure 4.18 Left ventricular, septal, and wall dimensions may also be measured from transverse images at the level of the chordae tendinae. Using a reference line connecting the chordae on each side of the chamber, draw a line perpendicular to it that bisects the ventricular cavity into symmetrical and equal halves. Use this line as the reference points for measurement. RV = right ventricle, IVS = interventricular septum, LV = left ventricle, LVW = left ventricular wall.

Wall and septal thicknesses are measured from either longor short-axis imaging planes along the same lines used to measure ventricular chamber dimensions. The trailing edge method is used for the septum, and the leading edge method is used for the wall.
Left ventricular length is a measurement that does not have a corresponding M-mode parameter. This measurement is obtained from the right parasternal long-axis four-chamber view or a modified right parasternal long-axis left ventricular outflow view where the left atrium is no longer visible and only a portion of the ascending aorta is seen. Both of these planes should have clear definition of the left ventricular apex. On the four-chamber plane, a line defining the mitral annulus is drawn (Figure 4.19). The measurement of left ventricular length is then made along a line connecting the apex to the point that bisects the annulus equally. On the modified view, two slightly different locations may be used to measure left ventricular length. A reference line defining the aortic annulus is drawn (Figure 4.20). One measurement extends from the apex of the left ventricle to a point midway across the aortic valve. Another measurement can be taken along a line that extends from the apex to the point where the aortic valve and mitral valve meet.
Figure 4.19 Right parasternal four-chamber views are used to measure ventricular length and atrial size. A line spanning the left atrial side of the mitral annulus is drawn for reference. Ventricular length is measured from the apex of the left ventricle to the midpoint of the reference line. Left atrial size is measured from anterior to posterior along a line parallel to the reference line and which bisects the atrium as closely as possible into equal halves. An apical basilar measurement of the left atrium may be made along a line that is perpendicular to the reference line and also divides the atrium as closely as possible into half. RV = right atrium, TV = tricuspid valve, RA = right atrium, LV = left atrium, MV = mitral valve, LA = left atrium, LVW = left ventricular wall.
Figure 4.20 A right parasternal long-axis left ventricular outflow view that is slightly modified so as not to visualize good mitral valves is used to measure ventricular length. A line extending across the aortic valve is used for reference. Ventricular length may be measured along a line connecting the apex of the chamber to the midpoint of the aortic valves or to the aortic mitral valve junction. RV = right ventricle, TV = tricuspid valve, RA = right atrium, IVS = interventricular septum, AO = aorta, LA = left atrium, LV = left ventricle, LVW = left ventricular wall.
Left parasternal apical four-chamber views are also used to measure left ventricular length (Figure

4.21). A reference line is drawn along the ventricular side of the mitral annulus. The length is measured along a line extending from the apex to a point that bisects the reference line in half.
Figure 4.21 The left parasternal apical four-chamber view may also be used to measure ventricular length. A line extending from the apex to the midpoint of a reference line drawn on the ventricular side of the mitral annulus is used for measurement. Left atrial size is measured from base to annulus perpendicular to the line defining the mitral annulus. Left trial width is measured along a line perpendicular to the base annulus measurement at the largest left atrial width. LV = left ventricle, RV = right ventricle, IVS = interventricular septum, MV = mitral valve, TV = tricuspid valve, LA = left atrium, RA = right atrium,IAS = interatrial septum.
Left Ventricular Mass
Cardiac hypertrophy usually involves an increase in left ventricular wall thickness. It is not always visibly apparent since there may be wall thinning as the heart dilates. This increase in mass can be quantified by several methods, including angiography, M-mode echocardiography and twodimensional echocardiography. M-mode echocardiographic methods rely on accurate measurement of wall and septal thicknesses at specified locations. This assumes a hypertrophy pattern that remains consistent throughout the heart. Two-dimensional assessment of left ventricular mass has proven to be superior to M-mode measurement of mass because the entire geometry of the heart is taken into consideration. M-mode assessment of mass will not be discussed in this chapter, but references are available if the reader wants to investigate this method of mass quantification (25–27). Twodimensional methods of determining mass have been tested in the dog and proven to be quite accurate with a correlation coefficient of .98 between echocardiographically determined ventricular mass and necropsy determined mass in dogs (28,29). The same formulas were applied to terminally ill people with abnormal cardiac dimensions, and the formulas estimated mass very accurately with an r value of
.93. Only in vitro mass determination has been assessed in the horse but the correlation was .96 (30).
Under the appropriate hypertrophic conditions, it is probably useful in both clinical and research applications.
There is no effect of sex on ventricular mass, but there is a significant curvilinear or second order correlation between body weight and ventricular mass in dogs (31). Mass determination is an involved process, and it is not routinely performed during a clinical exam. External and internal volumes of the heart are measured, and the difference between the two should equal myocardial volume. The myocardial volume is then multiplied by density in order to calculate ventricular mass (24).
Mass should remain constant throughout the cardiac cycles and does so with a high correlation (.92) between measurements taken in diastole and systole in the dog (29). Papillary muscles and trabeculae are easier to differentiate and eliminate in endocardial traces when they are made during diastole however. Measurements are taken in diastole just before atrial contraction. This creates the least amount of cardiac motion and the best visualization of muscle boundaries.
Only one method of mass determination using the long axis and transverse views will be described here, but two methods of measurement for mass determination have been studied in the dog. One is based on an assumption that the heart is shaped like a truncated ellipse (28,29). The other uses basically the same approach to mass determination but follows a simpler area length methodology (27). Neither is more accurate than the other.
The truncated ellipse has proven to be accurate in both normal and hypertrophied canine hearts and during both diastole and systole (Figure 4.22) (28,32). Volume is determined from the longest possible apical four-chamber view of the heart. This method of analysis requires measurements of chamber size to be taken along three directions on the apical four-chamber view. The minor axis is located at the tip of the papillary muscles at the point of chordal attachment (b). The long axis of the heart is divided into both a semi major (a) and a truncated semi major axis (d). The minor axis is the dividing line between the semi major axis and the truncated semi major axis. The minor axis is also represented by the diameter of the left ventricle on both longand short-axis views of the heart at the level of the chordae.
Figure 4.22 (A) Short-axis and (B) long-axis views of the heart are used to determine left ventricular mass based on the assumption that that heart is shaped like a truncated ellipse. Wall thickness (t) is derived from transverse sections at the level of the chordae tendinae by tracing epicardial and endocardial surfaces at end diastole and applying the equation as shown below (A). A truncated semimajor axis (d) and a full semimajor axis (a) are determined from the long-axis plane shown in (B). The semimajor axis is divided by b at the level of the papillary muscle—chordal junction. All values are inserted into the first equation shown below (B) to determine volume (v). Mass is calculated by multiplying volume by the specific gravity of myocardium (1.05 g/mL) using the second equation below (B). Adapted from Schiller NB, Skiôldebrand CG, Schiller EJ, et. al. Canine left ventricular mass estimation by two dimensional echocardiography. Circ 1983: 68;210–216.

In addition to the measurements of left ventricular length and width, wall thickness (t) is measured. On the transverse plane at the level of the tips of the papillary muscles, both the epicardial and endocardial surfaces are traced. The papillary muscles and any trabeculae are not included in the trace. Subtracting the systolic area from the diastolic area gives a mean wall thickness measurement. All the measurements are inserted into the equation shown in Figure 4.22 to calculate volume (V). The
equation calculates volume of the left ventricle when the epicardium is traced and volume of the ventricle when the endocardium is traced. Subtracting the two volumes results in volume of the ventricular myocardium. Mass is then calculated by multiplying the volume by myocardial specific gravity (Equation 4.1).
Equation 4.1 
The echocardiographically derived mass has an excellent correlation with post mortem mass (r =
.98) in dogs (27,33). Once echocardiographic mass is determined, the value is inserted into a regression equation that correlates echo-derived mass to actual post mortem mass as follows:
Equation 4.2 
where actual weight is in kg.
Transverse images of the horse’s heart are used to determine left ventricular volumes with a high level of correlation (.96) as discussed earlier. The volume is then multiplied by myocardial specific gravity in order to calculate left ventricular mass (Equation 4.1). These results were obtained in vitro (30).
Aorta and Left Atrium
Left atrial size can be measured from the right parasternal long-axis four-chamber view in the dog (Figure 4.19) (34). A reference line connecting the mitral annulus is drawn on the atrial side of the valve. The anterior posterior dimension of the left atrium is measured by drawing a line that as closely as possible bisects the atrium into equal halves and is parallel to the line defining the annulus. An apical basilar dimension may also be measured on two-dimensional images. This is done by drawing a line perpendicular to the line defining the annulus and again dividing the atrium as closely as possible into equal halves (Figure 4.19). The apical basilar measurement extends from the base of the atrium to the reference line and not to the valve leaflets themselves.
The left atrium in dogs may also be measured on left parasternal apical four-chamber views, which maximize left atrial size (Figure 4.21) (34). This plane may be slightly different than the one used to measure left ventricular length since each chamber should be maximized for the parameter to be measured. A line defining the mitral annulus on the atrial side is used as a reference for the other measuring points. The basal apical measurement is made from a line that as closely as possible divides the atrium into equal halves and is perpendicular to the reference line. The basal apical measurement starts at the base of the atrial septum and stops at the reference line. A lateral medial measurement can also be made. This is done from a line that divides the atrium into equal halves and is parallel to the reference line at the annulus.
The long-axis left ventricular inflow outflow view is used instead of the long-axis four-chamber view to measure left atrial size in the cat (35). The frame just before mitral valve opening is used. The largest left atrial dimension is measured along a line that is parallel to the mitral annulus (Figure 4.23).
Figure 4.23 Aortic root size from right parasternal long-axis views are made at both the level of the valve and at the maximum distance across the sinus of Valsalva. Left atrial size is measured at the largest LA dimension along a line that is parallel to the mitral annulus. RV = right ventricle, TV = tricuspid valve, RA = right atrium, IVS = interventricular septum, AOV = aortic valve, AO = aorta, MV = mitral valve, LA = left atrium, LV = left ventricle, LVW = left ventricular wall, RMPA = right main pulmonary artery.

The transverse image at the level of the aorta and left atrium is the most common imaging plane used to measure left atrial size in the dog and cat (34,35). All three aortic valve cusps must be seen with symmetry, in other words all cusps should be relatively equal in size. This assures that the image is as close to a true transverse imaging plane as possible. The left auricular appendage and atrial septum should also be clearly seen. The frame just after aortic valve closure is selected, and the left atrium is measured along a line that is an extension of the line that defines the junction between the noncoronary and left coronary cusps (Figure 4.24). The area of the left atrium may be obtained from any of these planes (Figures 4.24, 4.25). Trace the endocardial surface of the left atrium along the inside of the mitral valve and exclude the pulmonary veins.
2D Transverse Heart Base
Measurement of LA:AO
Image
All three aortic valve cusps seen
Good atrial septum seen
Good left auricle seen
First frame just after AO valve closes
Measurement Location
Measure AO along line defined by the noncoronary and right coronary cusps.
Measure LA along line defined by non coronary and left coronary cusps.
Internal dimensions
Figure 4.24 Area calculation of the aortic root is made at the level of the valves on transverse images. TV = tricuspid valve, RV = right ventricle, RA = right atrium, PV = pulmonic valve, IAS = interatrial septum, LA = left atrium, LAU = left auricle.

Figure 4.25 Left atrial area is measured by tracing the endocardial surface of the chamber from right parasternal four-chamber views or left parasternal apical four-chamber views. RV = right ventricle, TV = tricuspid valve, RA = right atrium, IVS = interventricular septum, MV = mitral valve, LA = left atrium, LV = left ventricle, LVW = left ventricular wall.

Aortic root measurements are made from a right parasternal long-axis view that maximizes the aorta at the expense of the left atrium (Figure 4.23). A well-defined aorta and two valve cusps should be seen. A line defining the annulus is used to measure the aortic diameter. Additionally, the distance across the sinus of Valsalva can also be measured. The largest dimension is selected and is measured along a line parallel to the one defining the aortic valve annulus.
The left parasternal long-axis left ventricular outflow view is also used to measure aortic root size. The annulus is measured on the aortic side of the valve, and this is also used as a reference line (Figure 4.26). The sinus of Valsalva is measured at its largest dimension in a line parallel to the reference line. The ascending aorta distal to the sinus may also be measured. Divide the measurement of the sinus of Valsalva in half and measure the ascending aorta that far away from the line that defined the measurement for the sinus.
Figure 4.26 Left parasternal images of the left ventricular outflow tract are also used to measure the aorta. In addition to measuring the distance at the level of the valves and the sinus of Valsalva, the ascending aorta is measured at a point distant to the sinus equal to half the measured size of the sinus. RV = right ventricle, PV = pulmonic valve, IVS = interventricular septum, AOV = aortic valve, AO = aorta, MV = mitral valve, LA = left atrium, LV = left ventricle, LVW = left ventricular wall.
Planimetry of the aorta is done on either the right or left parasternal transverse views of the aorta (Figure 4.24). Trace along the internal surface of the aorta at the level of the aortic valve cusps.
Right Ventricular Chamber
Measurement of right ventricular size is typically obtained from the apical four-chamber view. Measurements are made across the width of the tricuspid valve annulus and the mid ventricular chamber, and length is measured from the annulus to the apex (24). Normal reference ranges are
limited in animals, but linear changes in size can be used in the individual animal. Wall thickness is measured from parasternal two-dimensional four-chamber images at the level of the tricuspid valve chordae tendinae (24). Be careful not to include trabeculae.
Evaluation of Quantitative Measurements
Dogs
All parameters of ventricular size correlate to body surface area (BSA). Ratios of left atrium to aorta and wall thickness to chamber size do not correlate with body size, nor does any parameter of function (21). Reference values are in the appendices.
Systolic and diastolic dimensions derived from short-axis views tend to be slightly greater than those obtained from long-axis views, but the difference is not significant and the correlation between chamber sizes and wall thicknesses obtained from longversus short-axis images are high with correlation coefficients of .93 for diastolic dimensions, .88 for systolic dimensions, .95 for diastolic wall thickness, and .86 for systolic wall thickness. Septal thickness measurements also show no significant difference between imaging planes, but the correlation coefficients were slightly lower. There are also no significant differences between measurements taken from right or left parasternal imaging planes for the left atrium and aorta.
Ventricular lengths during diastole and systole show no significant differences between any of the three measuring techniques on right parasternal images. The right parasternal images were much better than left parasternal images for measuring length, however, since the left parasternal images tended to foreshorten the ventricular chamber.
Cats
Mean values from longand short-axis planes are not significantly different. There is no significant correlation between body surface area or weight and parameters of cardiac size in the cat (20). This is probably due to the small weight range within the adult cat population.
Two-dimensional and M-mode measurements in cats are very similar, but the closest relationship appears between measurements taken from two-dimensional short-axis measurements and M-mode values (20). M-modes in the reported study however were not obtained with two-dimensional guidance.
Horses
Two-dimensional measurements are available for the horse (36,37). One study validated the measurements for accuracy by postmortem echocardiographic measurement comparison (36). All values of echocardiographic size showed correlations greater than .87 with autopsy measurements. The second study found a significant correlation to body weight for the interventricular septum systolic thickness, aortic root dimension at end systole, chordal lumen of the left ventricle at end systole (37).
Parameters are measured by the same methods described for the dog in the following planes: right and left transverse planes of the left ventricle at the level of the papillary muscles and the chordae tendinae, left transverse images of the left ventricle at the level of the mitral valve and heart base with aorta, right-sided long-axis four-chamber, right-sided long-axis with left ventricular outflow, left-