


because the heart motion is too erratic as it swings within the pericardial sac (1,41,51). These changes all disappear after pericardiocentesis (41). The presence of cardiac tumors can also impair cardiac function if they are infiltrative in nature or produce arrhythmias (52).
Neoplasia as a Cause of Pericardial Effusion
Introduction
Cardiac neoplasia has a reported incidence of .19–3.1% of all canine cases presented to institutions. Hemangiosarcoma is reported with the highest frequency, 40–69%; chemodectomas are reported in 5– 17%; thyroid carcinomas, lymphosarcomas, and various less common neoplasias make up the rest of the cardiac tumors seen in dogs (30,53–56). Cardiac neoplasia is not common in cats, but of the reported cases, lymphosarcoma is the most common intrapericardial neoplasia, up to 30%, with other carcinomas, hemangiosarcomas, chemodectomas, and fibrosarcomas representing a low percentage (5,15,54,57). Echocardiography cannot actually identify the actual histological type of neoplasia, but the location and appearance of the mass tends to be highly suggestive of particular types of tumors (30,34,54,57).
The search for cardiac masses is easier when pericardial effusion is present. Masses may be found within the cardiac chambers, within the myocardium, or associated with the pericardial sac. The following intracardiac tumors have been reported: chondrosarcoma, fibroma, fibrosarcoma, hemangiosarcoma, hamartoma, mesenchymal tumor, myxoma, osteosarcoma, rhabdomyoma, rhabdomyosarcoma, ectopic thyroid tumor, spindle cell sarcoma, and undifferentiated sarcoma (58– 74). The right side of the heart is the most common location for masses in the dog while left ventricular and left atrial masses are much less common (52,54,65,75,76). Occasionally tumors may also be associated with the right and left ventricular outflow tracts (67,77). Diligently search in every possible cardiac plane for a potential mass. The animal should be scanned lying down from both sides of the thorax, and if a mass is not seen, continue the search with the animal standing and scan from both sides. Masses have been found simply by repositioning the animal into a standing position when no evidence of a mass was seen in lateral recumbency (6,11). Even then the absence of a mass does not rule out its presence especially when there is no pericardial effusion to highlight the auricular chambers and other structures at the base of the heart (1,2,78,79). Detection of masses with echocardiography has a sensitivity of between 16.7 and 80% (1,14,34,54,79,80). This variation may be dependent upon the presence of pericardial effusion and/or the skill of the echocardiographer. Discrete masses like hemangiosarcoma and chemodectoma are much easier to identify with echocardiography than more diffuse neoplasia such as mesothelioma and lymphosarcoma (39,81,82). Serial echocardiographic exams are sometimes necessary with recurrent pericardial effusion before some masses are large enough to be visualized (2,10,30,79,83,84). It is important to point out that the echocardiographic appearance of intracardiac tumors and intracardiac thrombi are very similar, and they cannot be differentiated using this imaging modality (85,86).
Unless the heart is scanned from both sides of the thorax when the animal is lying down and standing up, masses will be missed.
Aortic Body Tumors
There are many reports of aortic body tumors in dogs, but reports are rare in cats (23,54,87–90). These tumors develop from the chemoreceptor cells located at the heart base, around the aorta, and carotid bifurcation and are chemodectomas or nonchromaffin paragangliomas (54,91). At times chemodectomas are an incidental finding since dogs are symptomatic only when there is significant pericardial effusion, invasion into adjacent structures, or compression of adjacent structures (54,87,92–95). When pericardial effusion is present, it may be small or quite large in volume. These tumors are typically seen at the level of the aorta or pulmonary artery on long-axis or transverse views. On transverse views, the mass is seen around the aorta or pulmonary artery and between the pulmonary artery and right atrium, or along the aortic arch. It may be seen between the right auricular appendage and ascending aorta making it difficult to differentiate from a right auricular mass (87). The presence of a large tumor along the aortic arch will allow visualization of the arch and possibly the brachycephalic trunk as the mass wraps around these structures (10,78,90,96–98). Chemoreceptors rarely metastasize and are only locally invasive (54). Often it appears to invade the atria or the great vessels, but it may simply be in the field of view or compressing the atria (Figure 8.9). Deciding whether a mass is within the cardiac chambers or compressing the chambers is sometimes not possible. Heart base tumors on long-axis views are seen at the base of the heart around the aorta pushing into either atrium.
Figure 8.9 Heart base tumors are found along the aortic arch, pulmonary artery, and left atrium on two-dimensional images. This large mass (arrows) grew around the pulmonary artery along each side of the right main pulmonary artery and appears to invade the right and left atrium. (A) Right parasternal transverse image at the heart base, (B) right parasternal four chamber. RV = right ventricle, RA = right atrium, AO = aorta, LA = left atrium, LV = left ventricle, RMPA = right main pulmonary artery.

Heart base tumors are generally homogeneous in appearance with no hypoechoic areas within them, but there are exceptions. Small masses are usually oval or circular in shape, well defined, and localized. Large heart base masses have irregular boundaries and may diffusely invade the adjacent atria and ventricles (Figures 8.10, 8.11) (78,99). Some heart base tumors may be impossible to detect since they manifest themselves as thin small masses spread out over the surface of the aorta (84). The entire mass is rarely seen since the mass beyond the immediate cardiac boundaries is usually obscured by lung. The location of masses large enough to see are usually well defined however, and their accessibility for surgical removal can usually be determined (78).
Figure 8.10 Typical heart base masses grow along the aortic wall above the right main pulmonary artery branch (arrow) on echocardiographic images but may be seen anywhere around the heart base. AO = aorta, PA = pulmonary artery, RA = right atrium, RMPA = right main pulmonary artery, plane = right parasternal transverse heart base.

Figure 8.11 Although heart base masses are usually homogeneous in appearance, they may contain hypoechoic areas (arrow) similar to hemangiosarcoma. AO = aorta, PA = pulmonary artery, RA = right atrium, plane = right parasternal transverse heart base.
Do not confuse collapsed lung with a mass at the heart base or mediastinum. The lung will maintain a wedge shape, float within the pleural fluid, and may contain small hyperechoic areas (Figures 8.12, 8.13).
Figure 8.12 Collapsed lung (arrow) should not be mistaken for a mass at the heart base or mediastinum. The lung will maintain a wedge shape and may contain hyperechoic areas within it. PLE = pleural effusion.
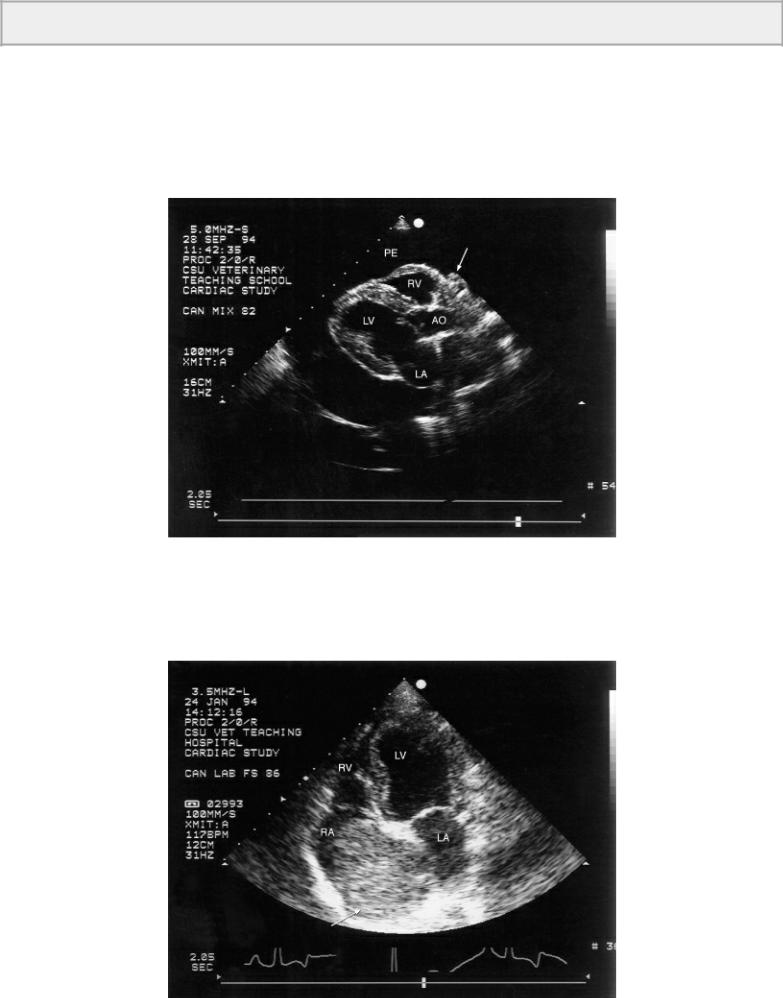
Figure 8.13 Diffuse areas of poor image at the heart base (arrow) should not be misinterpreted as a tumor. A mass should be examined and seen in several planes to be confident about its presence. PE = pericardial effusion, RV = right ventricle, LV = left ventricle, plane = right parasternal four chamber.
Other Heart Base Masses
Right ventricular tumor associated with the pulmonic valve and pulmonary artery has been reported (Figure 8.14). These have been identified as myxomas, thyroid carcinoma, neurofibromas, chondrosarcomas, and fibrosarcomas (38,100). When associated with the pulmonary valve and right ventricular outflow tract, they have created right ventricular outflow obstruction to varying degrees. Right heart failure as well as decreased preload to the left ventricle may develop if occlusion is severe. The masses may be fairly immobile and adherent to the wall of the outflow tract or pulmonary artery, or move freely with the pulmonic valve depending on the extent of adherence to the walls of the outflow tract.

Figure 8.14 This tumor (arrow) attached to the pulmonic valve was fairly mobile and moved with the valve but obstructed flow from the right ventricle. The right heart was enlarged secondary to the obstruction, and tricuspid insufficiency was significant. RA = right atrium, RV = right ventricle, PA = pulmonary artery, AO = aorta, plane = right parasternal transverse heart base.
A small proportion of heart base masses are the result of ectopic thyroid tumors (carcinomas, adenocarcinomas) (2,54,101–104). They can be found on echocardiographic images around the heart base or between the aorta and pulmonary artery or atrial chambers.
Hemangiosarcoma
Hemangiosarcomas arise from vascular endothelium and can be found anywhere in the body, but the heart is a frequent site where it is typically associated with the right atrium or auricle (11,35,67,75,105,106). It is commonly found within the right atrial wall or as an auricular mass extending into the pericardial space or into the auricular lumen (Figures 8.15, 8.16, 8.17, 8.18, 8.19, 8.20, 8.21). It may involve the right ventricular wall, invade the pericardial sac, or rarely the left ventricular chamber (Figures 8.22, 8.23) (10,35,52,75,79). Hemangiosarcomas usually have smooth, well-defined boundaries; rarely are they irregular masses. They are typically heterogeneous containing many hypoechoic areas (Figure 8.24). High-resolution transducers are necessary to resolve diffuse hemangiosarcoma involving just the wall of the ventricle or atrium. Although hemangiosarcoma may be found in many different imaging planes, and each view should be interrogated, the left cranial longaxis view of the right auricular appendage is probably the most useful one for identifying cardiac hemangiosarcoma (78). Echocardiographic detection of hemangiosarcoma in the dog has a reported sensitivity of 48–69% (1,79,80,107). This includes repeat examinations in several dogs when no mass was found on initial exams. Effusion is not necessary for the diagnosis of hemangiosarcoma, but effusion does help highlight the areas of interest especially the right auricle. Right auricular tumors are the most difficult to visualize, and small tumors may only be identified when effusion is present and the right auricle floats within the pericardial fluid on left cranial long-axis views of the right atrium and auricle (1,7,79).
Hemangiosarcomas are best seen on left parasternal cranial long-axis views of the right atrium and auricle.
Figure 8.15 Hemangiosarcoma is typically found within the right auricle and atrium. When pericardial effusion is present, the right auricle and most masses can be seen on right parasternal images such as this one (arrow). The left parasternal view of the right auricle should also be examined. PE = pericardial effusion, RV = right ventricle, AO = aorta, LV = left ventricle, LA = left atrium.
Figure 8.16 Large hemangiosarcomas are easy to find on almost any view. Here the mass fills the right atrial chamber on an apical four-chamber plane (arrow). RV = right ventricle, LV = left ventricle, RA = right atrium, LA = left atrium.

Figure 8.17 Hemangiosarcoma is commonly found in or around the right auricular appendage as it is here (arrow). PE = pericardial effusion, RV = right ventricle, TV = tricuspid valve, LV = left ventricle, RA = right atrium, plane = left cranial long axis of the right auricle.
Figure 8.18 Pericardial effusion allows the right auricle to be seen well as it floats within the pericardial fluid. The mass (arrow) attached to the outside of this auricle may not have been detected without the effusion to highlight it. RA = right atrium, RAU = right auricle, PE = pericardial effusion, plane = left parasternal right auricle.
Figure 8.19 A mass attached to the right atrial wall is hemangiosarcoma in this dog. PE = pericardial effusion, RV = right ventricle, TV = tricuspid valve, AO = aorta, RA = right atrium, plane = left cranial transverse view.

Figure 8.20 A pericardial effusion highlights the mass found within the right ventricular and atrial walls at the right atrioventricular junction. PE = pericardial effusion, RV = right ventricle, RA = right atrium, RAA = right atrial appendage, LV = left ventricle, LA = left atrium, plane = right parasternal four chamber.
Figure 8.21 This large hemangiosarcoma containing many hypoechoic areas within it is seen in the right auricular appendage. There is no pericardial effusion associated with this mass. RV = right ventricle, LV = left ventricle, TV = tricuspid valve, RA = right atrium, RAA = right atrial appendage, plane = left cranial long axis of the right auricle.

Figure 8.22 Less commonly hemangiosarcoma may be seen within the right atrial and ventricular walls. (A) Here the irregular wall of the right atrial chamber is abnormal (arrows). (B) Farther down toward the right ventricular apex is a more distinct mass (arrow) with characteristic hemangiosarcoma appearance. Notice the irregular right ventricular wall from tumor invasion. RV = right ventricle, RA = right atrium, AO = aorta, plane = left parasternal apical four chamber.

Figure 8.23 Hemangiosarcoma is seen within the left interventricular septum of this dog’s heart. LV = left ventricle, plane = right parasternal transverse left ventricle.

Figure 8.24 This tumor within the right ventricular chamber contains many hypoechoic areas within it characteristic of hemangiosarcoma. AO = aorta, PA = pulmonary artery, LA = left atrium, RV = right ventricle, plane = right parasternal heart base.
Lymphosarcoma
Lymphosarcoma is an infiltrative type of cardiac neoplasia seen most often in cats and cows but is occasionally reported in the dog and horse (1,39,53,57,108–116). Up to 30% of the cardiac neoplasias in cats are lymphosarcoma (57). Although cardiac neoplasia is rare in the cat, it is reported to be present in 10–15% of cats with lymphoma and even higher in cats with feline leukemia virus (53,57). Infiltrative diseases in man are usually associated with restrictive cardiomyopathy with the most common underlying cause being amyloid deposition (117). Infiltrative disease resulting in restrictive physiology has been documented in the cat secondary to lymphosarcoma and endomyocardial fibrosis

(24,118,119).
Lymphosarcoma involving the heart is perceived on echocardiographic images as hypertrophied hypokinetic muscle with or without areas of increased echogenicity (113). There may be associated pericardial effusion resulting in tamponade (111,113). Lymphosarcoma involving only the pericardium is reported with resulting tamponade and no visible echocardiographic abnormalities of the pericardial sac (Figures 8.25, 8.26) (39,120).
Lymphosarcoma is usually an infiltrative disease. The myocardium appears hypertrophied and hypokinetic.
Figure 8.25 Lymphosarcoma infiltrated the septum of this dog creating asymmetric hypertrophy. Function of the heart was also compromised. RV = right ventricle, VS = ventricular septum, LV = left ventricle, LVW = left ventricular free wall.
Figure 8.26 Lymphosarcoma of the heart looks like hypertrophied hypokinetic muscle with or without areas of increased echogenicity. This cat with lymphosarcoma of the heart has increased thickness of the ventricular and atrial walls (arrows) and increased echogenicity of the muscle. RV = right ventricle, LV = left ventricle, LA = left atrium, PE = pericardial effusion, plane = right parasternal four-chamber view.

Other Intracardiac Neoplasia
Lipomas
Lipomas, though generally found in subcutaneous tissues, have been seen within the heart and pericardial sac of dogs and horses (86,121,122). Primary cardiac lipomas consist of adipose cells that originate in the epicardium, myocardium, or endocardium. They can infiltrate the walls of the heart and create thrombosis within the vessels entering or leaving the heart (121,123). Lipomas within the pericardial sac may be attached to the surface of the heart by a stalk and can become quite large without elevating pressure significantly presumably due to their slow growth and soft consistency (86,122). In man, patients with cardiac lipomas are usually asymptomatic, but there are occasional reports of arrhythmia, obstruction of flow into or out of the heart (121).
Rhabdomyosarcoma
Rhabdomyosarcomas, striated muscle tumors, are rare in all species. They are usually infiltrative in nature but can extend into the cardiac chambers as polyp-like growth (124). Rhabdomyosarcoma in the dog has been seen in the right ventricular and atrial walls with partial obstruction of the right ventricular inflow and outflow tracts. They can have irregular borders (53,55,70,71,125–130).
Myxoma and Myxosarcoma
Myxomas, though not common in dogs, are benign masses typically found within the left atrial chamber of the heart (67,131,132). They are attached to the wall of the left atrium by a pedicle and are easily removed. Echocardiographically they appear uniform in tissue character with smooth borders (133). Paraganglioma has been found within the left atrial chamber of the dog and echocardiographically cannot be differentiated from myxoma (134). They may obstruct flow into or out of the left atrial chamber. Myxosarcomas however are a rare malignant often infiltrative endocardial growths of mesenchymal origin that may involve the pulmonary artery, right ventricle and atrium, right ventricular outflow tract, left ventricle, and pericardial sac (135–138). They are common in rabbits and poultry but rare in dogs (137). Echocardiographically they are usually multilobed and