

Onco-emergencies |
63 |
|
|
Atul Kulkarni and Vandana Agarwal |
|
A 58-year-old male patient with metastatic renal cell carcinoma presented with lethargy, confusion, anorexia, nausea, and constipation. He was polyuric and polydipsic over the past few days.
63.1Hypercalcemia
Oncological emergencies such as hypercalcemia, tumor lysis syndrome, superior vena cava syndrome, and spinal cord compression are occasionally seen as an intercurrent problem or presenting manifestation in certain cancers.
Step 1: Resuscitate
•Hydration is of utmost importance in these patients, and intravenous saline should be given rapidly once hypercalcemia is confirmed (refer to Chap. 78).
Step 2: Send investigations
•Measure ionized serum calcium (arterial or venous).
•If total serum calcium is measured, correct for the albumin level. Corrected calcium = measured total calcium + [0.8 × (4.0−albumin)].
•Also, check serum creatinine, electrolytes, and alkaline phosphatase.
•A low serum chloride level (<100 mEq/L) suggests hypercalcemia of malignancy.
•ECG abnormalities reflect altered transmembrane potentials, affecting conduction such as QT interval shortening (common) and QRS interval lengthening (high levels). T waves may flatten or invert, and a variable degree of heart block may develop.
A. Kulkarni, M.D. (*) • V. Agarwal, M.D., F.R.C.A.
Department of Anaesthesia, Critical Care and Pain, Tata Memorial Hospital, Mumbai, India
e-mail: kaivalyaak@yahoo.co.in
R. Chawla and S. Todi (eds.), ICU Protocols: A stepwise approach, |
499 |
DOI 10.1007/978-81-322-0535-7_63, © Springer India 2012 |
|
500 |
A. Kulkarni and V. Agarwal |
|
|
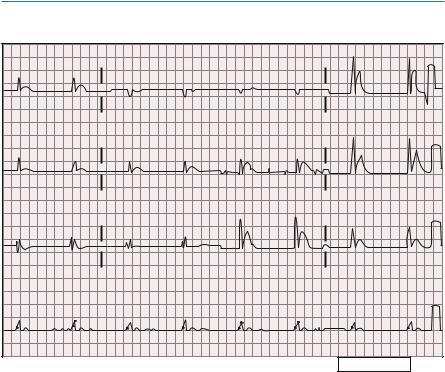
63.2ECG Changes in Hypercalcemia
I |
|
aVR |
|
V1 |
|
V4 |
|
II |
|
aVL |
|
V2 |
|
V5 |
|
III |
|
aVF |
|
V3 |
|
V6 |
|
II |
|
|
|
|
|
|
|
Device |
Speed |
25 mm / sec |
L1 ab |
10 aa / aV |
Chest |
10 aa / aV 40-0.5-4.0 W1 V |
1w0701 |
The above ECG shows a short QT interval with hardly any ST segment, characteristic of hypercalcemia. In this tracing, the QRS complexes are wide, indicative of an intraventricular conduction defect. No P waves are evident, and this is most likely a junctional escape rhythm.
Step 3: Infuse fluid
•Severe hypercalcemia is usually associated with marked hypovolemia.
•Give 500–1,000 mL of normal saline in the first hour and continue at a lower rate until volume repletion is achieved and urine output is established.
•In patients with impaired cardiorespiratory and renal function, aggressive fluid resuscitation should be done with close hemodynamic monitoring.
Step 4: Start diuretics after fluid repletion
•Consider loop diuretics only when euvolemia is achieved, as hypovolemia causes renal hypoperfusion hampering calcium excretion.
•Diuretics are specifically useful if features of hypervolemia, secondary to aggressive fluid resuscitation, develop.
63 Onco-emergencies |
501 |
|
|
|
|
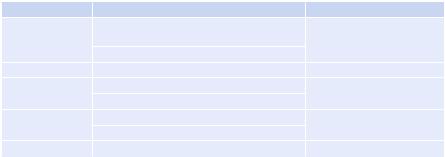
Table 63.1 Treatment for hypercalcemia |
|
|
Intervention |
Dosage |
Comment |
Normal saline |
250–500 mL/h until euvolemic, thereafter |
Caution in patients with |
|
100–150 mL/h IV, may require 3–4 L |
congestive heart failure |
|
Keep urine output 100–150 mL/h |
|
Furosemide |
20–40 mg IV |
After volume correction |
Bisphosphonates |
Pamidronate: 60–90 mg IV over 2–24 hours |
Caution in renal impairment |
|
Zoledronic acid: 4 mg IV over 15 min |
|
Glucocorticoids |
Prednisolone: 60 mg/day PO |
Hyperglycemia, |
|
Hydrocortisone: 100 mg IV every 6 h |
immunosuppression |
Calcitonin |
4–8 IU/kg SC or IM every 12 h |
Rapid onset but short lived |
Step 5: Start specific therapy
•Bisphosphonates block osteoclastic bone resorption.
•Use zoledronic acid with caution in patients with renal impairment, and adjust the dose according to creatinine clearance (Table 63.1).
•Subcutaneous or intramuscular calcitonin lowers calcium levels quickly, but the effect is short lived.
•In some patients with lymphomas, particularly Hodgkin’s disease, hypercalce-
mia is caused by elevated levels of vitamin D (1,25(OH)2D); glucocorticoids are particularly effective.
Step 6: Decrease intake
•Eliminate dietary sources of calcium.
•Discontinue medications such as thiazide diuretics (increase the reabsorption of calcium) and vitamin D that increase the calcium level.
Step 7: Consider dialysis
•Dialysis should be considered for patients with renal failure and/or congestive heart failure when aggressive hydration and bisphosphonates cannot be used safely.
Step 8: Treat the cause
•Treat the malignancy with chemotherapy and radiation to control the hypercalcemia if possible.
Step 9: Evaluate prognosis
•In patients with advanced malignancy, hypercalcemia may commonly occur.
•In such circumstances, it may be appropriate, ethical, and humane to institute only comfort measures if no effective treatment for malignancy exists (Fig. 63.1).
63 Onco-emergencies |
503 |
|
|
•Obtain electrocardiogram to rule out serious arrhythmias and conduction abnormalities.
•Tumor lysis is associated with malignancies like acute lymphoblastic leukemia or Burkitt’s lymphoma with high tumor burden and responds rapidly to chemotherapy.
•It usually follows chemotherapy, but may occur after radiation, corticosteroid therapy, or chemoembolization and rarely spontaneously.
•Check urine output and renal function.
Step 3: Start hydration
•A high infusion rate of fluids is appropriate.
•Patients with high risk of tumor lysis syndrome should have aggressive volume replacement as a preventive measure prior to chemotherapy.
•Infuse isotonic fluid at a rate of 200–300 mL/h.
•Volume should be adapted for the patient’s age, cardiac function, and urine output.
•Increasing the urinary flow rate is the most effective strategy for preventing urate-induced obstructive uropathy.
•Urine output should be maintained within a range of 80–100 mL/m2/h (4–6 mL/ kg/h if <10 kg).
•Urine-specific gravity should be maintained at £1.010.
Step 4: Use diuretics cautiously
•Maintain adequate urine output.
•It is contraindicated if hypovolemia or obstructive uropathy exists.
Step 5: Alkalinization of the urine
•This was recommended earlier but is controversial as it can lead to the formation of urinary xanthine crystals.
•This may cause obstruction of renal tubules if allopurinol is used concurrently.
•It is not recommended with recombinant urate oxidase (rasburicase).
Step 6: Start allopurinol
•Purine catabolism results in the production of hypoxanthine and xanthine, which are metabolized to uric acid via the enzymatic action of xanthine oxidase.
•This pathway can be blocked by the use of allopurinol, a hypoxanthine analog that competitively inhibits xanthine oxidase.
•Start allopurinol PO at 600 mg/day if uric acid is less than 8 mg/dL.
•Allopurinol should be started prior to chemotherapy.
•After about 2–3 days, allopurinol therapy results in increased excretion of both hypoxanthine, which is more soluble than uric acid, and xanthine, which is less soluble than uric acid.
•A marked increase in xanthine excretion can occur when allopurinol is given for prevention of tumor lysis syndrome and may lead to acute renal failure or xanthine stones.