


Chapter 4 Equipment, Instruments, and Materials |
55 |
Fig. 4.32. Binocular loupes with light source, adapted to a headband
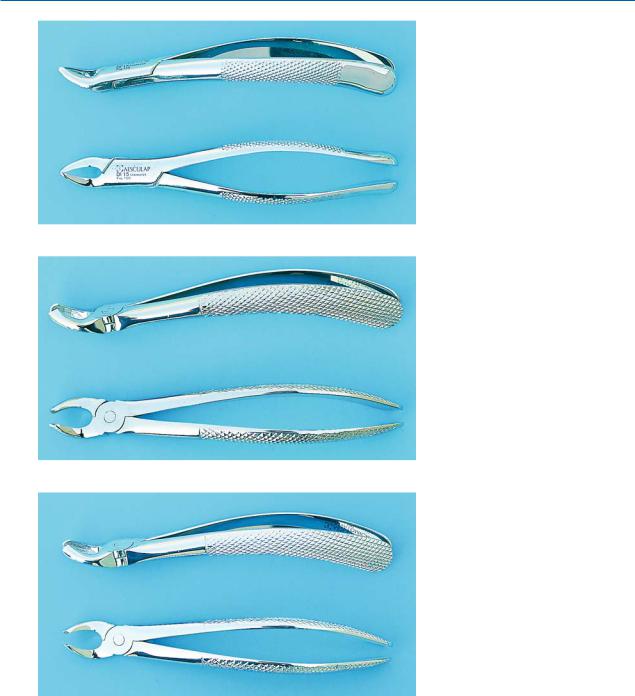
Fig. 4.34. Maxillary extraction forceps used for the six anterior teeth of the maxilla (superior and side view)
suring good vision of the surgical field (Figs. 4.32, 4.33). This system also has a light source that projects intense light into difficult areas of the surgical field (e.g., posterior teeth), where vision by means of standard lighting is not satisfactory.
4.19
Extraction Forceps
The simple intra-alveolar extraction is accomplished with the help of extraction forceps and elevators. Each extraction forceps is composed of two parts, which are crossed in such a way that they make up one instrument when used to extract a tooth. The basic components of the extraction forceps are the handle, which is
Fig. 4.33. Binocular loupes with light source, adapted to eyeglass frames
above the hinge, and the beaks, which are below the hinge (Fig. 4.34). The instrument is held in the hand by the handle, upon which pressure is exerted during the extraction. The beaks are the functional component of the forceps and grasp the tooth at the cervical region and remove it from the alveolar socket.
Because tooth anatomy varies, extraction forceps with specially designed beaks have been manufactured, so that they may be used for specific teeth. So, according to the size and shape of the handles and beaks, the following types exist.
Maxillary Extraction Forceps for the Six Anterior Teeth of the Maxilla. Beaks that are found on the same level as the handles characterize these forceps, and the beaks are concave and not pointed (Fig. 4.34).
56 F. D. Fragiskos
Maxillary Universal Forceps or No. 150 Forceps. The forceps used for premolars have a slightly curved shape and look like an “S.” Holding the forceps in the hand, the concave part of the curved part of the handle faces the palm, while the concave part of the beaks is turned upwards. The ends of the beaks of the forceps are concave and are not pointed (Fig. 4.35). These forceps may also be used for extraction of the six anterior teeth of the upper jaw.
Fig. 4.35. Maxillary universal forceps or no. 150 forceps (mainly used for upper premolars)
Fig. 4.36. Maxillary right molar forceps, for the first and second upper molars of the right side
Fig. 4.37. Maxillary left molar forceps, for the first and second upper molars of the left side
Maxillary Molar Forceps, for the First and Second Molar. There are two of these forceps: one for the left and one for the right side. Just like the previously mentioned forceps, they have a slightly curved shape that looks like an “S” (Figs. 4.36, 4.37). The buccal beak of each forceps has a pointed design, which fits into the buccal bifurcation of the two buccal roots, while the palatal beak is concave and fits into the convex surface of the palatal root.

Chapter 4 Equipment, Instruments, and Materials |
57 |
Fig. 4.38. Maxillary third molar forceps
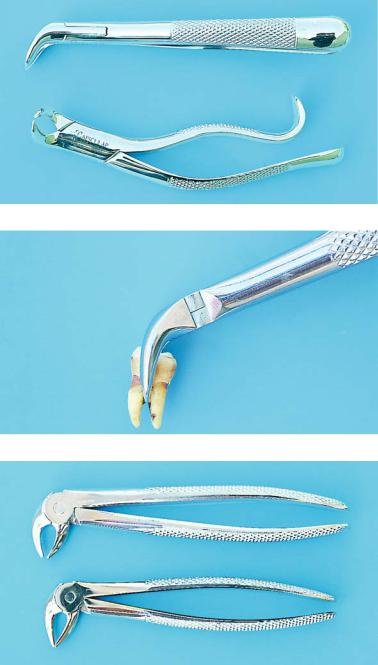
Fig. 4.39. Maxillary root tip forceps
Maxillary Third Molar Forceps. These forceps have a slightly curved shape, just like the aforementioned forceps, and are the longest forceps, due to the posterior position of the third molar (Fig. 4.38). Because this tooth varies in shape and size, the beaks of the forceps are concave and smooth (without pointed ends), so that these forceps may be used for extraction of both the left and right third molar of the upper jaw.
Maxillary Cowhorn Molar Forceps. The upper cowhorn forceps are a variation of the maxillary molar forceps. The beaks of this type of forceps have sharply pointed ends, which fit into the trifurcation of the roots of the molars. They are primarily used for extraction of teeth with severely decayed crowns, because when they are used to extract intact teeth, they may fracture the buccal alveolar bone due to the large amount of force they generate.
Maxillary Root Tip Forceps. The handles of the root tip forceps are straight, while the beaks are narrow and angle-shaped. The ends of the beaks are concave and without a pointed design (Fig. 4.39).
Mandibular Forceps for Anterior Teeth and Premolars or Mandibular Universal Forceps or No. 151 Forceps. Unlike the maxillary forceps, the beaks and handles of these forceps face the same direction, creating an arch. When the forceps are held in the hand, the concave part of the arch of the handles faces the palm, while the beaks obviously face downward. The ends of the beaks are concave, without pointed ends (Fig. 4.40).
The no. 151 forceps are used for extraction of the six anterior teeth and the four premolars of the lower jaw.
Mandibular Molar Forceps. These forceps are used for both sides of the jaw and have straight handles while the beaks are curved at approximately a right angle compared to the handles. Both beaks of the forceps have pointed ends, which fit into the bifurcation of the roots buccally and lingually (Fig. 4.41). These forceps are used for the removal of both the first and second molar of the right and left side of the lower jaw.
58 F. D. Fragiskos
Fig. 4.40. Mandibular forceps for anterior teeth and premolars of the mandible or mandibular universal forceps or
no. 151 forceps
Fig. 4.41. Mandibular molar forceps
Fig. 4.42. Mandibular third molar forceps
Mandibular Third Molar Forceps. These forceps also have straight handles, while the beaks, just like those of the first and second molar forceps, are curved at a right angle compared to the handles. The beaks are a little longer compared to the previous forceps, due to the posterior position of the third molar in the dental arch (Fig. 4.42). Because this tooth varies in size and shape and because there is usually no root bifurcation, the ends of the beaks of the forceps are concave without a pointed design.
Mandibular Cowhorn Molar Forceps. The lower cowhorn forceps or no. 23 forceps are a variation of the mandibular molar forceps (Fig. 4.43). In comparison to the standard forceps, the beaks have a semicircular shape with sharply pointed ends so that they can fit into the bifurcation of the roots and firmly grasp the tooth (Fig. 4.44). Owing to the function of these forceps, tooth extraction may be achieved quite easily as long as the roots are not curved. With the beaks of the forceps grasping the crown of the molar and the
Chapter 4 Equipment, Instruments, and Materials |
59 |
Fig. 4.43. Mandibular cowhorn molar forceps for sectioning roots. They are used for extracting molars with intact crowns, and also when only sectioning of roots is necessary
Fig. 4.44. Mandibular cowhorn forceps adapted to molars
Fig. 4.45. English-style forceps with the hinge in the vertical direction
sharp ends fitting into the root bifurcation, the surgeon squeezes the handles and, using small buccolingual movements, slides the tooth out of the socket.
Also, the cowhorn forceps are very useful for sectioning roots of posterior teeth in the lower jaw, when their crowns are severely decayed. After grasping the roots, the teeth are easily sectioned after applying pressure at the bifurcation point.
Vertical Hinge Forceps. These English-style forceps differ from the aforementioned forceps in that their hinges have a vertical direction (Fig. 4.45). Their use is limited, because large amounts of force can be generated during extraction with this type of forceps, so that if the bone is not elastic, there is increased risk of fracture of the alveolar bone.