

|
|
Chapter 12 |
|
|
|
|
Surgical Treatment |
12 |
|
of Radicular Cysts |
|
|
C. Alexandridis |
|
|
|
|
Radicular (periapical) cysts are pathological cavities, lined with epithelium, and contain fluid or semi-fluid material.
They are the most common cystic lesions of the jaws and originate from the epithelial remnants of
Malassez rests, which are stimulated after inflammation at the apices of nonvital teeth.
Diagnosis of radicular cysts is based on clinical and radiographic examination, as well as aspiration of the contents of the cystic sac.
12.1
Clinical Presentation
The majority of radicular cysts are asymptomatic, especially those small in size. They are discovered after radiographic examination, unless they are suppurated, whereupon pain as well as other symptoms occur. Large cysts present swelling buccally and more rarely lingually or palatally. This swelling is due to expansion of the buccal cortical plate, which becomes thinned and may demonstrate a crackling sound (crepitus). If the bone is completely destroyed, the cyst is connected to the periosteum and the mucosa in this area looks bluish-red.
12.2
Radiographic Examination
Radiographically, radicular cysts present as osteolytic or radiolucent lesions (round or oval in shape) with well-defined radiopaque borders, unless they have been infected, whereupon the radiopaque periphery does not exist.
12.3
Aspiration of Contents of Cystic Sac
In addition to the clinical and radiographic examination, aspiration of the contents of the cystic sac may be
a valuable diagnostic aid. In cysts whose size is larger than 1.5–2 cm, thin or thick fluid may be aspirated, which precludes the presence of other more solid lesions.
12.4
Surgical Technique
Two techniques are employed in clinical practice for the surgical removal of cysts: enucleation and marsupialization.
Enucleation. This technique involves complete removal of the cystic sac and healing of the wound by primary intention. This is the most satisfactory method of treatment of a cyst and is indicated in all cases where cysts are involved, whose wall may be removed without damaging adjacent teeth and other anatomic structures.
The surgical procedure for treatment of a cyst with enucleation includes the following steps:
ΟReflection of a mucoperiosteal flap.
ΟRemoval of bone and exposure of part of the cyst.
ΟEnucleation of the cystic sac.
ΟCare of the wound and suturing.
After taking a radiograph to determine the exact localization and size of the lesion, a trapezoidal flap is created, whose extent must ensure adequate access and visualization of the surgical field (Figs. 12.1– 12.4).
After reflection of the mucoperiosteum, the bone covering the lesion is evaluated, which, as mentioned above, may be normal, thinned, or completely destroyed.
In normal bone, a round bur is used to remove a portion of the buccal cortical plate covering the cyst, and, depending on its extent, a rongeur may be used to enlarge the osseous window created (Figs. 12.5, 12.6).
The osseous window must be large enough so that all parts of the cystic cavity may be accessed and removed without particular difficulty.
302 C. Alexandridis
If the bony wall is thinned or perforated, it is removed peripherally with a rongeur, until it reaches compact bone. A curette is used for enucleation of small cysts, while for larger cysts, the broad end of a periosteal elevator is preferred, which is placed inside the cavity pressing gently between the cystic wall and bone, while the cyst is carefully grasped with forceps (Fig. 12.7).
After removal of the cysts, a curette is used to inspect the cavity for the presence of remnants of the cyst, and copious irrigation with saline solution and suturing of the flap follow (Figs. 12.8–12.10).
The surgical technique for removal of mandibular cysts is exactly the same as that described above
(Figs. 12.11–12.18).
Marsupialization. This method is usually employed for the removal of large cysts and entails opening a surgical window at an appropriate site above the lesion.
Surgical Removal of Maxillary Cyst
In order to create the surgical window, initially a circular incision is made, which includes the mucoperiosteum, the underlying perforated (usually) bone, and the respective wall of the cystic sac (Figs. 12.19– 12.23). After this procedure, the contents of the cyst are evacuated, and interrupted sutures are placed around the periphery of the cyst, suturing the mucoperiosteum and the cystic wall together (Fig. 12.24).
Afterwards, the cystic cavity is irrigated with saline solution and packed with iodoform gauze (Figs. 12.25, 12.26), which is removed a week later together with the sutures. During that period, the wound margins will have healed, establishing permanent communication.
Irrigation of the cystic cavity is performed several times daily, keeping it clean of food debris and averting a potential infection.
Healing of the wound is by secondary intention, and the epithelium of the cyst is thus transformed into oral mucosa.
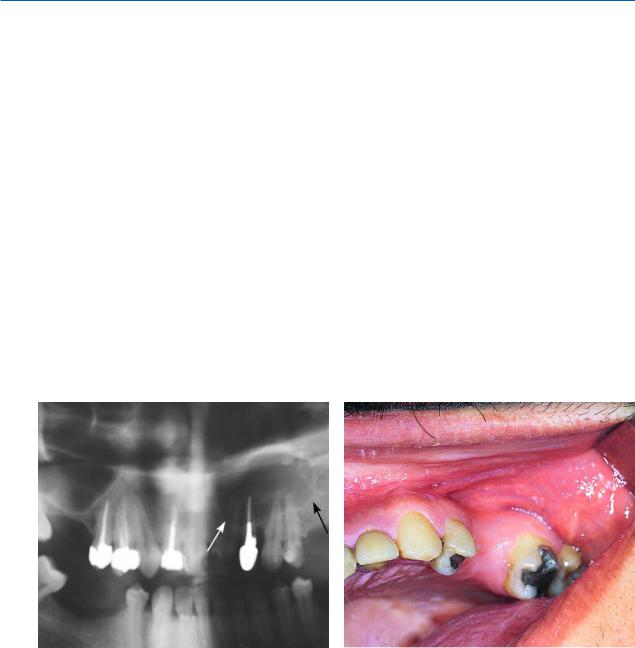
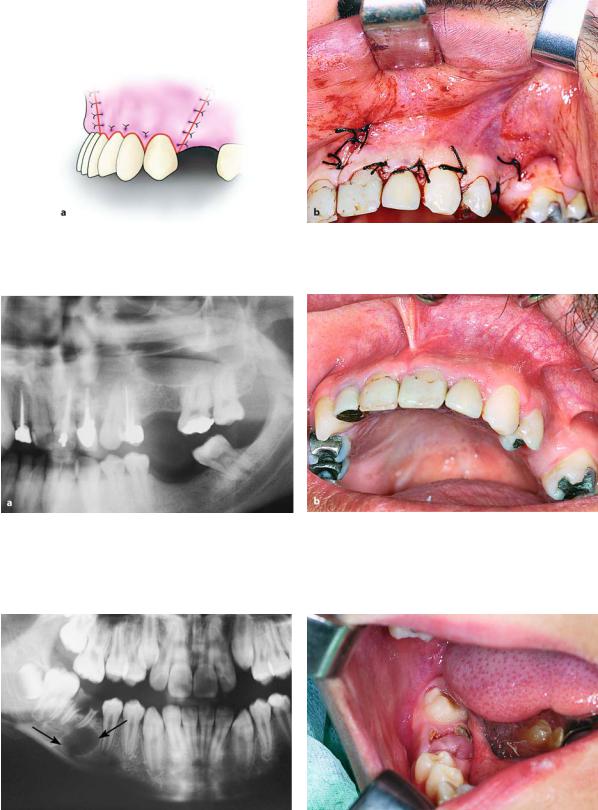
Fig. 12.1. Panoramic radiograph showing an extensive ra- Fig. 12.2. Clinical photograph of case of Fig. 12.1 dicular lesion at the region of teeth 22, 23, 24
Chapter 12 Surgical Treatment of Radicular Cysts |
303 |
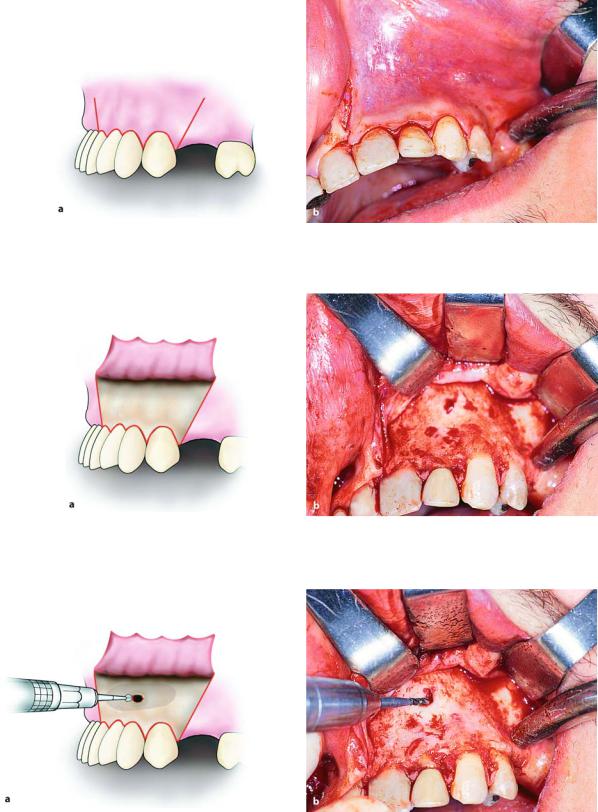
Fig. 12.3 a, b. Removal of maxillary cyst, with labial access. Incision for creating a trapezoidal flap. a Diagrammatic illustration. b Clinical photograph
Fig. 12.4 a, b. Reflection of flap and exposure of surgical field. a Diagrammatic illustration. b Clinical photograph
Fig. 12.5 a,b. Removal of bone at the labial aspect respective to the lesion. a Diagrammatic illustration. b Clinical photograph
304 C. Alexandridis
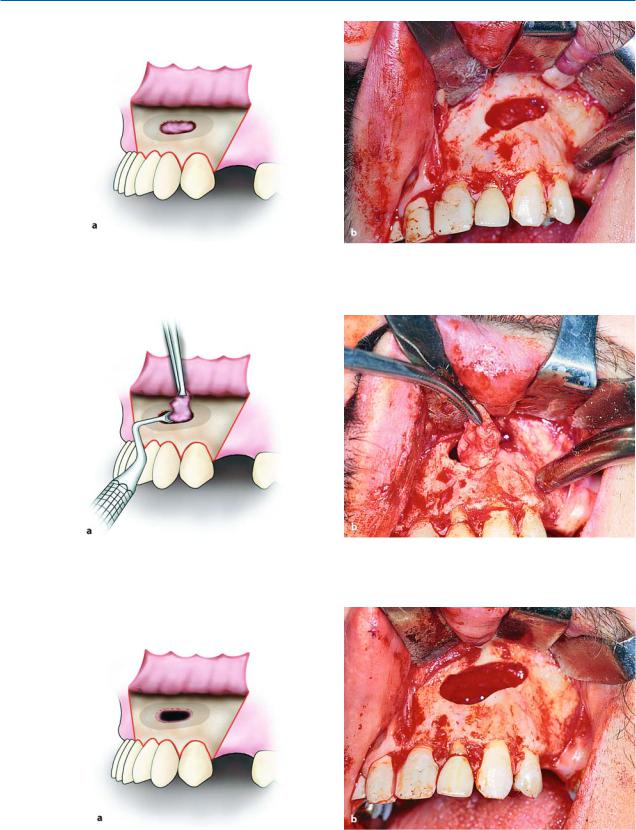
Fig. 12.6 a, b. Osseous window created to expose part of the lesion. a Diagrammatic illustration. b Clinical photograph
Fig. 12.7 a, b. Removal of cyst from bony cavity, using hemostat and curette. a Diagrammatic illustration. b Clinical photograph
Fig. 12.8 a,b. Surgical field after removal of lesion. a Diagrammatic illustration. b Clinical photograph
Chapter 12 Surgical Treatment of Radicular Cysts |
305 |
Fig. 12.9 a, b. Operation site after placement of sutures. a Diagrammatic illustration. b Clinical photograph
Fig. 12.10 a, b. Panoramic radiograph (a) and clinical photograph (b) of the area taken 2 months after the surgical procedure
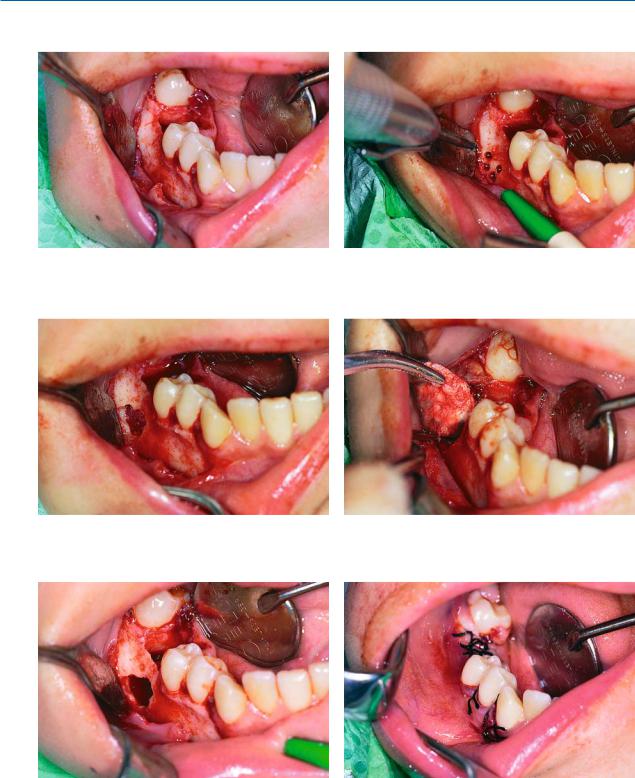
Surgical Removal of Mandibular Cyst
Fig. 12.11. Radiograph showing radicular lesion at area of Fig. 12.12. Clinical photograph of case of Fig. 12.11 mandibular first molar
306 C. Alexandridis
Fig. 12.13. Incision and reflection of mucoperiosteum |
Fig. 12.14. Holes drilled for removal of buccal alveolar |
|
plate |
Fig. 12.15. Osseous window completed, after joining of |
Fig. 12.16. Removal of lesion with help of hemostat and |
holes with fissure bur |
curette |
Fig. 12.17. Surgical field after removal of lesion |
Fig. 12.18. Suturing of wound with interrupted sutures |

Chapter 12 Surgical Treatment of Radicular Cysts |
307 |
Marsupialization of Cyst
Fig. 12.19. Radiograph showing extensive mandibular cyst. The marsupialization method is indicated for its treatment
Fig. 12.21. Exposure of buccal cortical plate and removal of portion of bone with round bur
Fig. 12.20. Treatment of mandibular cyst with marsupialization method. Circular incision includes mucosa and periosteum
Fig. 12.22. Enlargement of osseous window with rongeur
Fig. 12.23. Exposure of cyst after removal of bone |
Fig. 12.24. Suturing of wound margins with cystic wall |