

Chapter 14
Surgical Treatment |
14 |
of Salivary Gland Lesions |
F. D. Fragiskos
The most common surgical procedures for lesions associated with salivary glands and which may be performed with local anesthesia at the dental office are the removal of sialoliths from the ducts of glands and the removal of retention cysts.
14.1
Removal of Sialolith from Duct of Submandibular Gland
Sialolithiasis may occur in the ducts of large salivary glands or in the parenchyma of the glands themselves.
Of these glands, the submandibular is the most common site of occurrence (70–80%) compared to the parotid and sublingual glands. Fifty per cent of sialoliths
(stones) of the submandibular gland are located at the anterior portion and the middle of the gland, another 35% at its posterior portion, and the remaining 15% inside the gland itself. Sialolithiasis is the most common cause of inflammation of the gland, resulting in sialadenitis. If this condition is not treated, it becomes chronic with frequent recurrences, and may lead to destruction of the gland.
The main symptoms characterizing obstruction of the duct are pain and transient swelling of the respective salivary gland during meals. These symptoms are the result of increased saliva production during mastication, which – understandably enough, due to obstruction of the duct – is not secreted into the oral cavity.
The first clinical symptom is acute pain that occurs at the region of the gland and which is usually milder in the case of partial obstruction and more severe when obstruction is complete. Many times, the pain reflects to the floor of the mouth, tongue, pharynx, and cervical area. Swelling of the gland follows, which, depending on the amount of obstruction, gradually subsides after mealtimes.
Diagnosis is made based on clinical and radiographic data. In between meals, redness and slight swelling at the mucosa are observed, along the duct. The presence of a sialolith is also confirmed by bimanual palpation. More specifically, the index finger of one
hand is placed at the floor of the mouth, while the fingers of the other hand are placed at the submandibular area, simultaneously palpating the duct of the submandibular salivary gland in a posteroanterior direction.
With this manipulation, a hard, semi-round moveable swelling presenting tenderness is ascertained. A fundamental diagnostic aid is the occlusal radiograph. In difficult and doubtful situations, a sialogram and ultrasonic examination are considered necessary.
Treatment is surgical and consists of excision of the sialolith from the duct.
Surgical Technique. The case presented involves a sialolith located inside the duct of the submandibular salivary gland (Figs. 14.1–14.3 a). The procedure for its removal is as follows. After local anesthesia, an incision is made on the mucosa of the floor of the mouth
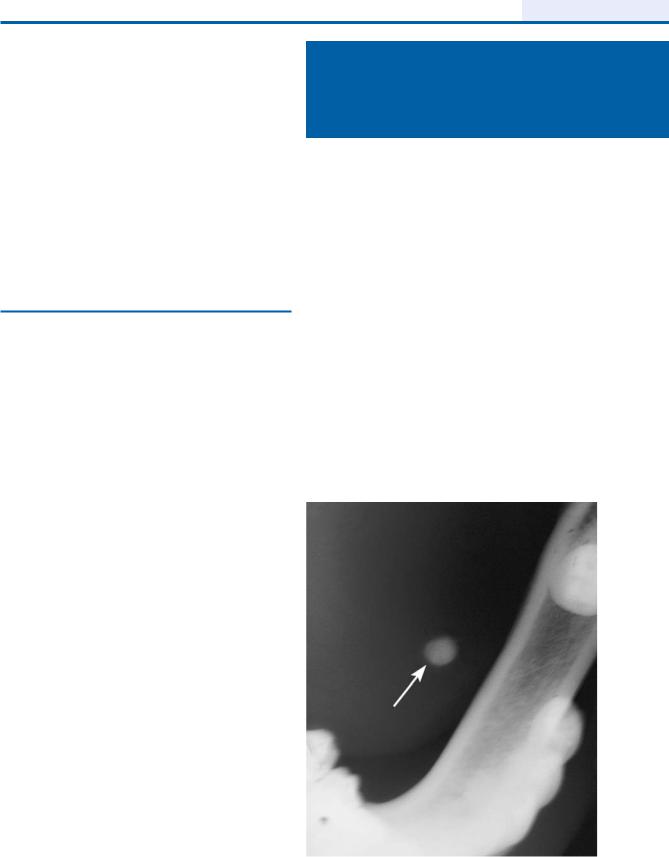
Fig. 14.1. Occlusal radiograph showing sialolith in duct of submandibular salivary gland
328 F. D. Fragiskos
Fig. 14.2. Clinical photograph of case shown in Fig. 14.1. Arrow points to swelling as a result of the sialolith
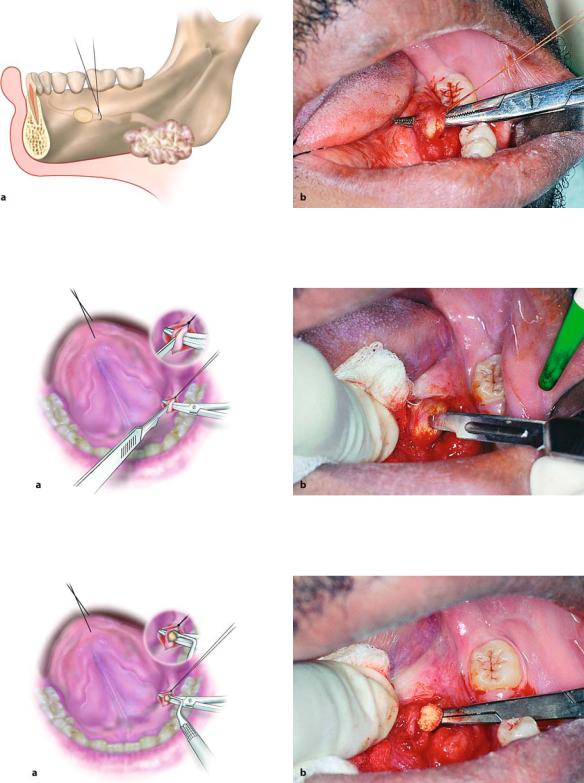
along the length of the duct, while the floor of the mouth is extraorally simultaneously pushed upwards. The incision is 1–1.5 cm long and is made exactly over the position of the sialolith (Fig. 14.3 b). After localization and preparation of the duct, a traction suture is placed underneath the duct and posterior to the sialolith, to facilitate the incision procedure, but also to avoid distant displacement of the sialolith (Figs. 14.4,
14.5) (ligation may be also performed at the beginning, before the incision, as is shown in Fig. 14.3 b). Afterwards, the suture is retracted upwards and an incision is made at the duct along its long axis, resulting in spontaneous exposure of the sialolith, which is removed with a curette or a hemostat (Figs. 14.6, 14.7). The wound is then sutured with interrupted sutures at the mucosa only, without including the duct (Figs. 14.8, 14.9).
Fig. 14.3 a, b. Diagrammatic illustrations, showing: a the position of the sialolith in the duct, and b the incision on the mucosa, underneath which the sialolith is localized
Fig. 14.4 a, b. Exposure and preparation of the duct of the salivary gland after incision on mucosa. a Diagrammatic illustration. b Clinical photograph
Chapter 14 Surgical Treatment of Salivary Gland Lesions |
329 |
Fig. 14.5 a, b. Ligation of the duct posterior to the sialolith, in order to avoid distal displacement of the sialolith during surgical procedure. a Diagrammatic illustration. b Clinical photograph
Fig. 14.6 a, b. Incision along the length of the duct where the sialolith is located. a Diagrammatic illustration. b Clinical photograph
Fig. 14.7 a, b. Exposure and removal of the sialolith using hemostat and curette. a Diagrammatic illustration. b Clinical photograph

330 F. D. Fragiskos
Fig. 14.8 a, b. Operation site after suturing. a Diagrammatic illustration. b Clinical photograph. The orifice of the duct is not sutured
Fig. 14.9. Sialolith after removal
During the surgical procedure, the dentist must pay particular attention to the proper preparation of the duct, in order to avoid risk of severance, which would result in chronic sialadenitis. Also, care must be taken when the sialolith is located in a posterior area, where the duct is in close proximity to the lingual nerve. Careful manipulations must also be performed in such a case with the aforementioned technique, because injury or severance of the nerve would result in permanent hypesthesia or anesthesia of the respective half of the tongue.
14.2
Removal of Mucus Cysts
The most common surgical procedures for removal of mucus cysts and which may be performed with local anesthesia at the dental office involve mucoceles and ranulas. These are both retention phenomena, essentially differing in localization only.
14.2.1 Mucocele
“Mucocele” is the clinical term used to describe the mucus extravasation phenomenon, as well as the mucus retention cyst. The mucus extravasation phenomenon is due to trauma of the minor salivary gland excretory duct, resulting in retention of saliva in the surrounding tissues, and is essentially classified as a false cyst, since it lacks an epithelial lining. This lesion mainly occurs at the mucosa of the lower lip, due to frequent biting, and may be superficial or deep in the tissues. The mucus retention cyst differs from the mucus extravasation phenomenon in that it is the result of obstruction of salivary flow, as well as being surrounded by granulation tissue.
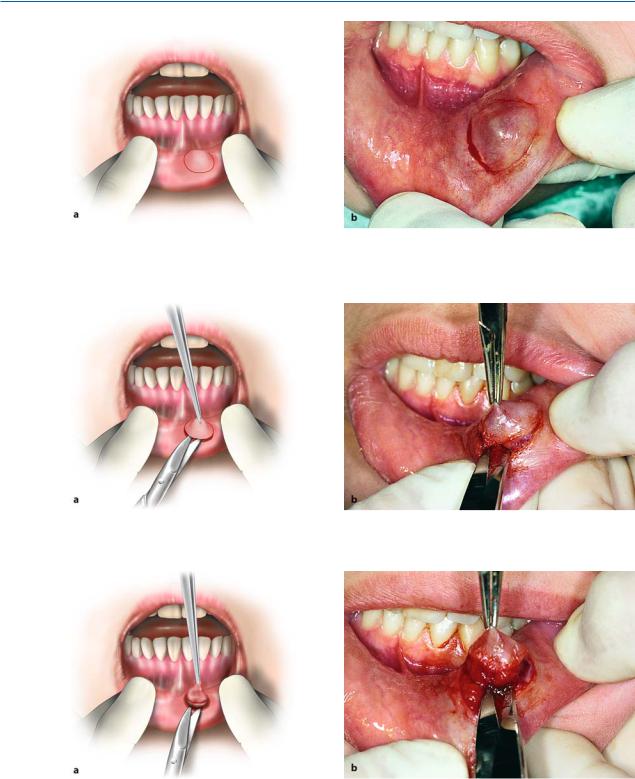
Clinically, the lesion is painless and presents as a smooth round or oval swelling that fluctuates. Its color is normal or slightly bluish, and its size ranges from a few millimeters up to 2 cm (Fig. 14.10).
Treatment is surgical and entails excision of the lesion.
Surgical Technique. After local anesthesia, an elliptical incision is made on the mucosa around the cyst, in order to facilitate dissection of the lesion (Figs. 14.11– 14.13). The superior wall of the cyst is grasped with a hemostat together with the overlying mucosa and is separated from the surrounding tissues (Figs. 14.14, 14.15) using scissors. During dissection care must be taken, because the cyst may easily rupture and shrivel, which will make removal difficult. In such a case, preparation may be facilitated if gauze is placed inside the erupted cystic cavity, so that the cavity is again expanded and restored to its previous condition. After removal of the lesion, the mucosa of the wound mar-

Chapter 14 Surgical Treatment of Salivary Gland Lesions |
331 |
Fig. 14.10 a, b. Mucus extravasation phenomenon of the lower lip (mucocele). a Diagrammatic illustration. b Clinical photograph
Fig. 14.11 a, b. Peripheral infiltration in normal tissues surrounding lesion
Fig. 14.12 a, b. Elliptical incision around cyst with scalpel. a Diagrammatic illustration. b Clinical photograph
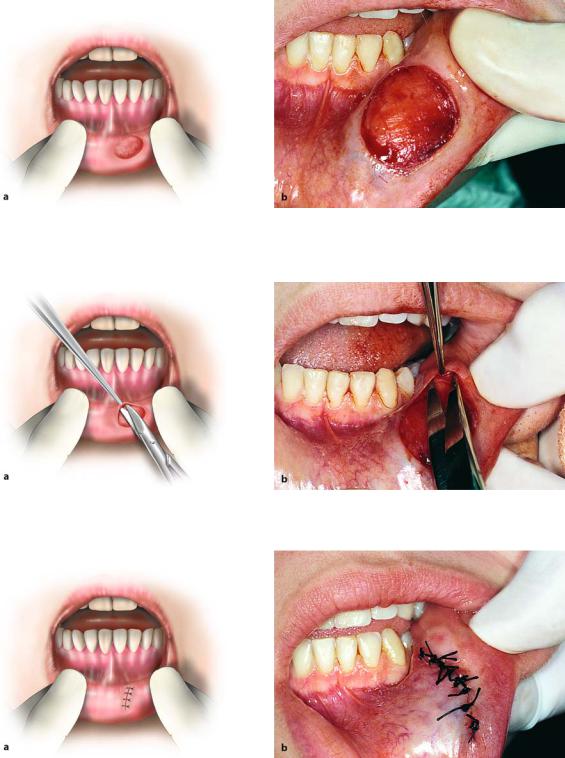
gins are undermined and superficially sutured (only at the mucosa), avoiding injury to the underlying salivary glands (Figs. 14.16–14.18).
332 F. D. Fragiskos
Fig. 14.13 a, b. Diagrammatic illustration (a) and clinical photograph (b) of completed incision
Fig. 14.14 a, b. Lesion is grasped with hemostat and is dissected using scissors. a Diagrammatic illustration. b Clinical photograph
Fig. 14.15 a, b. Final step in removal of cyst from underlying soft tissues. a Diagrammatic illustration. b Clinical photograph
Chapter 14 Surgical Treatment of Salivary Gland Lesions |
333 |
Fig. 14.16 a, b. Surgical field after removal of lesion. a Diagrammatic illustration. b Clinical photograph
Fig. 14.17 a, b. Undermining of mucosa of wound margins with blunt scissors. a Diagrammatic illustration. b Clinical photograph
Fig. 14.18 a, b. Operation site after placement of sutures. a Diagrammatic illustration. b Clinical photograph
334 F. D. Fragiskos
14.2.2 Ranula
This is essentially a retention cyst that is due to obstruction or trauma of the duct of the sublingual or submandibular salivary gland, resulting in extravasation and retention of mucus, thus presenting as a mucus retention cyst and the mucus extravasation phenomenon, respectively. The ranula is located in the floor of the mouth and is usually unilateral, with a diameter ranging 1–3 cm.
Clinically, it presents as a soft fluctuant swelling with a normal or bluish hue, and resembles a frog’s belly (Fig. 14.19). It develops gradually and, depending on its size, may cause medial and superior deviation
of the tongue, creating problems during speech, mastication, and deglutition. If it is large in size, it may progress in the deep tissues and cross the midline while projecting submandibularly and posteriorly. The wall of the cyst is very thin, and, when ruptured, extravasation of inspissated mucin occurs, resulting in shriveling of the cavity after evacuation of its contents.
The ranula is treated surgically, principally with the method of marsupialization.
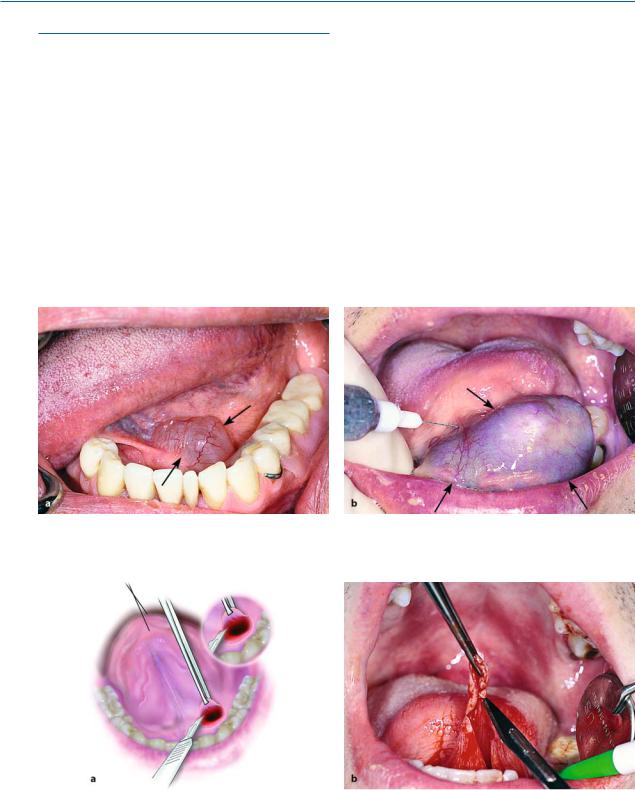
Surgical Technique. After local anesthesia, the superior wall of the cyst is grasped with a hemostat and a circular incision is made, which includes the oral mucosa covering the lesion together with its superior wall (Fig. 14.20). After aspiration of the contents, the margins of the mucosa are sutured with the margins of the
Fig. 14.19 a, b. Two cases of ranula, located at the left side of the floor of the mouth. a Small-sized lesion. b Large lesion
Fig. 14.20 a, b. Excision of portion of lesion includes the overlying oral mucosa and superficial wall of cyst. a Diagrammatic illustration. b Clinical photograph