


Chapter 6 Surgical Tooth Extraction |
99 |
6.2 Contraindications
The contraindications for a surgical extraction are as follows:
ΟAsymptomatic fractured root tips, whose pulp was vital, located deep in the socket. The extraction of such root tips should not be considered, especially in older patients, when:
–There is a risk of serious local complications, such as the dislodging of a root tip into the maxillary sinus or injury of the inferior alveolar nerve, mental nerve, or lingual nerve.
–A large part of the alveolar process needs to be removed.
–There are serious health problems present. If a patient with health problems needs to have a surgical extraction, then it must be performed with the cooperation of the treating physician and only if the general status of the patient has improved; the necessary preventive measures must also be taken.
6.3
Steps of Surgical Extraction
The surgical extraction techniques for single-rooted and multi-rooted teeth are similar, and include the following steps:
1.Creation of a flap.
2.Removal of bone and exposure of an adequate part of the root.
3.Extraction of the tooth or root with elevators or forceps.
4.Postoperative care of wound and suturing.
The surgical extraction involves teeth with intact crowns, roots and root tips, and presents certain characteristics in each of these cases.
6.4
Surgical Extraction of Teeth with Intact Crown
6.4.1
Extraction of Multi-Rooted Tooth
The removal of a single-rooted or multi-rooted tooth with an intact crown is achieved with the simple extraction technique and is usually very easy. There are certain situations, though, when the extraction requires a surgical approach, in order to avoid undesirable complications. The procedure for these cases is as follows. When the extraction involves a multi-rooted maxillary tooth, an envelope flap is created and the buccal plate is removed using a round bur, as far as the root bifurcation. The two buccal roots are sectioned after a groove is created using a fissure bur, and the crown together with the palatal root is then removed
(Fig. 6.17). The two other roots are then removed separately, preferably using a straight elevator or root tip forceps.
6.4.2
Extraction of an Intact Tooth
with Hypercementosis of the Root Tip
If an extraction is indicated for a tooth that has hypercementosis at the root tip, then it must be performed using the surgical technique. Otherwise, as already mentioned, fracture of the root tip is inevitable. The procedure used for such cases generally is described below:
ΟWhen the tooth to be extracted is single-rooted
(Fig. 6.18 a), an L-shaped flap is initially created, and the bone covering the buccal surface of the root is then removed. The extraction is performed easily towards the buccal side that is no longer covered by bone, using forceps or elevators (Fig. 6.18 b).
100 F. D. Fragiskos
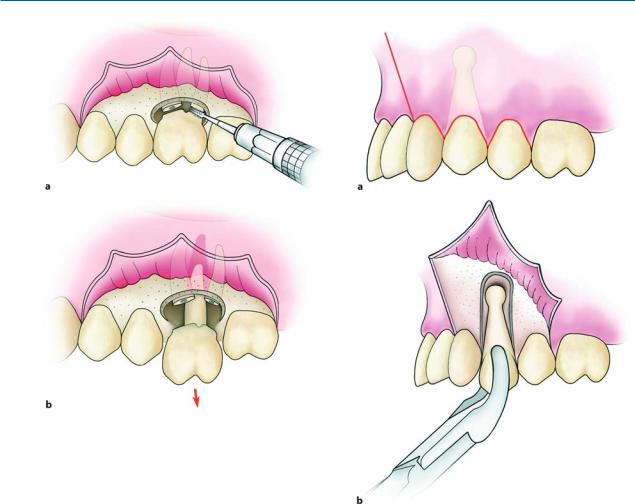
Fig. 6.17 a, b. Steps in the surgical extraction of an intact maxillary first molar. Reflection of the envelope flap, sectioning of two buccal roots from the crown (a), removal of the crown together with the palatal root, and then finally removal of the mesial and distal roots (b)
Fig. 6.18 a, b. Diagrammatic illustrations showing the steps in the surgical extraction of a single-rooted tooth with hypercementosis at the root tip. An L-shaped incision is made and the flap is reflected. The buccal plate covering the surface of the root is removed, and the tooth is extracted using forceps
ΟWhen the tooth to be extracted is multi-rooted with hypercementosis at the root tip (Fig. 6.19 a), at first an envelope flap is created, and the buccal bone is removed to just below the root bifurcation. The roots are separated, after a vertical groove is created on the crown of the tooth using a fissure bur, which extends as far as the intraradicular bone (Fig. 6.19 b). After this procedure, the mesial part is removed
first (root and crown) using forceps or an elevator (Fig. 6.20). Afterwards, the intraradicular bone is removed using a round bur, and the socket is widened along the length of the root (Fig. 6.21). After this widening, the distal part, which includes the bulbous root tip, is easily removed using forceps, a straight elevator or an elevator with T-shaped handles (Fig. 6.22).
Chapter 6 Surgical Tooth Extraction |
101 |
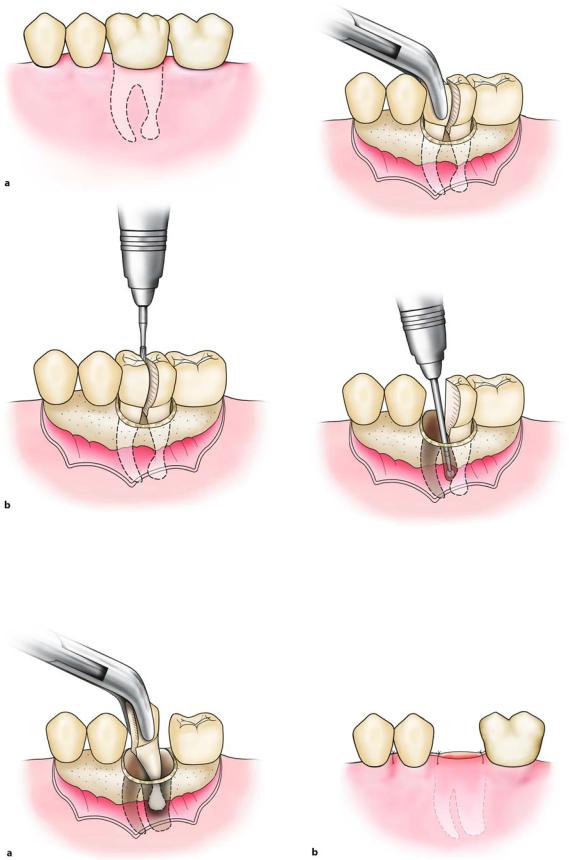
Fig. 6.19 a, b. Surgical extraction of a mandibular molar with hypercementosis at the distal root tip. The envelope flap is reflected, part of the buccal plate is removed, and the tooth is sectioned buccolingually at the crown as far as the intraradicular bone
Fig. 6.20. Extraction of the mesial portion of the tooth, which includes the crown and root
Fig. 6.21. Widening of the alveolus with a round bur, so that removal of the root is possible without fracturing the bulbous root tip
Fig. 6.22 a,b. a Extraction of the distal portion of the tooth using forceps after creating a pathway for removal. b Suturing of the flap using interrupted sutures
102 F. D. Fragiskos
6.4.3
Extraction of Deciduous Molar
that Embraces Crown of Permanent Tooth
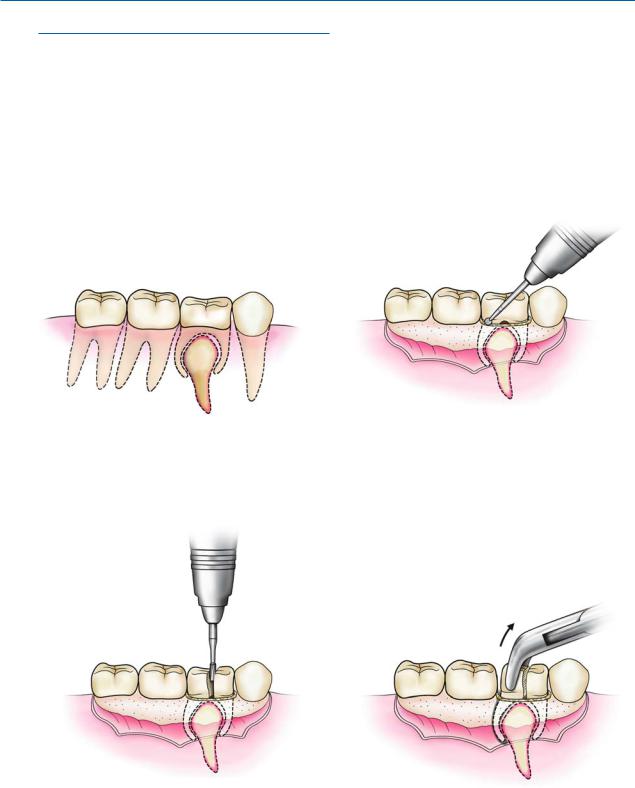
If an extraction is indicated for a deciduous molar and if examination of the radiograph reveals that the roots of the deciduous molar embrace the crown of the succedaneous premolar (Fig. 6.23), it must be removed
surgically using the following steps. First an envelope flap is created and then buccal bone is removed as far as the root bifurcation using a round bur (Fig. 6.24). Afterwards, the roots are separated with a vertical deep groove on the crown of the tooth using a fissure bur, and the distal part of the tooth is first removed using forceps, and then the mesial part (Figs. 6.25– 6.27). The flap is repositioned and sutured using interrupted sutures (Fig. 6.28).
Fig. 6.23. Deciduous molar, whose roots embrace the crown of the succedaneous premolar
Fig. 6.24. Envelope flap created and bone removed as far as the root bifurcation
Fig. 6.25. Roots of the molar sectioned with a perpendicu- |
Fig. 6.26. Removal of the distal portion of the tooth, which |
lar groove on the crown, which extends as far as the intra- |
includes the crown and root, using forceps |
radicular bone |
|
Chapter 6 Surgical Tooth Extraction |
103 |
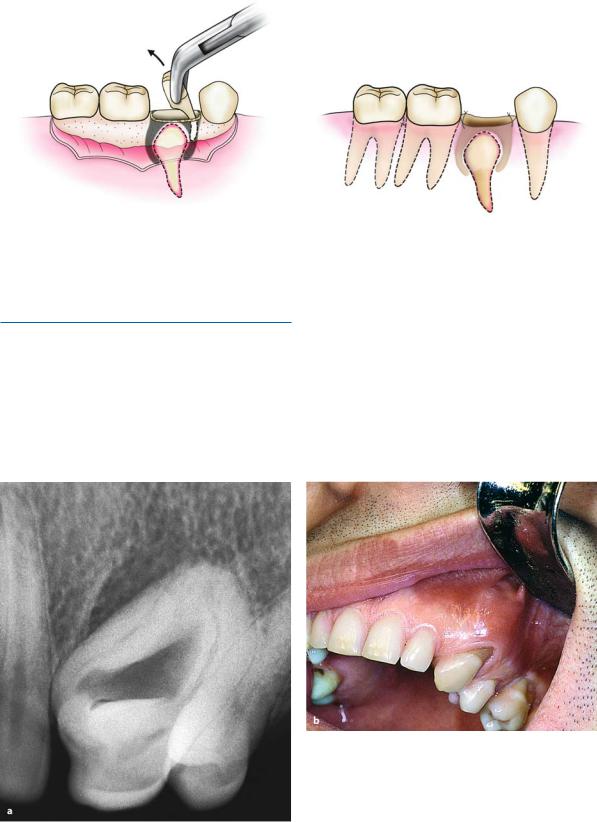
Fig. 6.27. Removal of the mesial portion of the tooth, which includes the crown and root
6.4.4
Extraction of Ankylosed Tooth
In the case of ankylosis of the tooth, and especially if dental dysplasia is also present (e.g., dens in dente), as shown in Fig. 6.29, the simple technique to extract the tooth must not be attempted, because there is a risk of
Fig. 6.28. Suturing of the flap with interrupted sutures
fracturing a large part of the buccal alveolar bone. The technique used to remove the tooth is usually as follows. After the creation of a trapezoidal flap, the buccal bone is removed around the tooth using a fissure bur. Using a chisel, the tooth is then carefully removed together with the ankylosed portion of the buccal alveolar bone. The socket is cared for and suturing of the flap follows (Figs. 6.30–6.33).
Fig. 6.29 a,b. Radiograph (a) and clinical photograph (b) of a maxillary canine with dens in dente. A surgical technique is indicated for its removal