

Chapter 10 Preprosthetic Surgery |
261 |
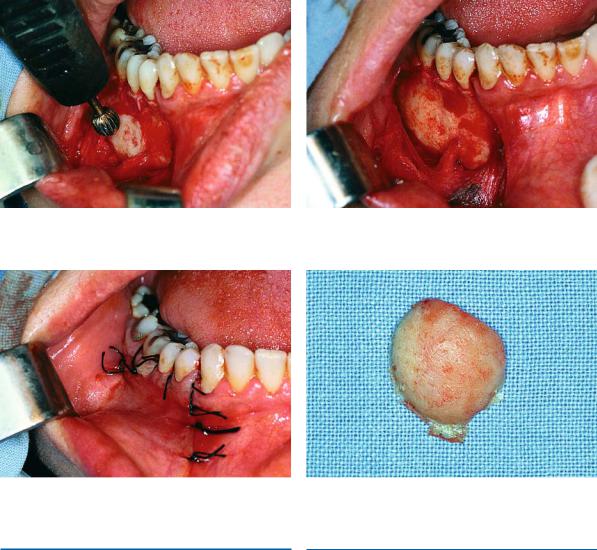
Fig. 10.68. Smoothing of the bone surface with a bone bur |
Fig. 10.69. Surgical field after removal of the exostosis and |
|
smoothing of the area |
Fig. 10.70. Operation site after suturing |
Fig. 10.71. Exostosis after removal |
10.2 |
10.2.1 |
Soft Tissue Lesions or Abnormalities |
Frenectomy |
Lesions or abnormalities associated with soft tissues and which require alteration are also classified into two categories:
a.Congenital abnormalities, such as a hypertrophic frenum, etc.
b.Abnormalities created after the use of dentures
(e.g., fibrous hyperplasia of the mucosa), and other causes.
In many cases, the placement of a complete denture of the maxilla, or orthodontic procedures in younger persons requires the removal of the labial frenum, especially if it is hypertrophic (Fig. 10.72). Also, in the mandible, the lingual frenum may create problems, causing partial or complete ankyloglossia (Fig. 10.73).
This case is due to attachment of the frenum to the floor of the mouth or to the alveolar mucosa. It may even be the result of an extremely short frenum that is connected to the tip of the tongue. Ankyloglossia greatly limits movements of the tongue, resulting in speech difficulties.

262 F. D. Fragiskos
Fig. 10.72. Hypertrophic maxillary labial frenum
10.2.1.1
Maxillary Labial Frenectomy
Excision of the labial frenum is easy, within the reach of the general practitioner, and may be performed with various techniques. The method usually employed is that of excision using two hemostats. In this case, the procedure used is as follows. After local anesthesia, the lip is pulled upwards, and the frenum is grasped using two curved hemostats, which are positioned at the superior and inferior margins (Figs. 10.74, 10.75).
Fig. 10.73. Ankyloglossia as a result of a short frenum
The lip is then further retracted and a thin scalpel blade incises the tissue found behind the hemostat, first behind the lower hemostat and then behind the upper hemostat (Figs. 10.76–10.78).
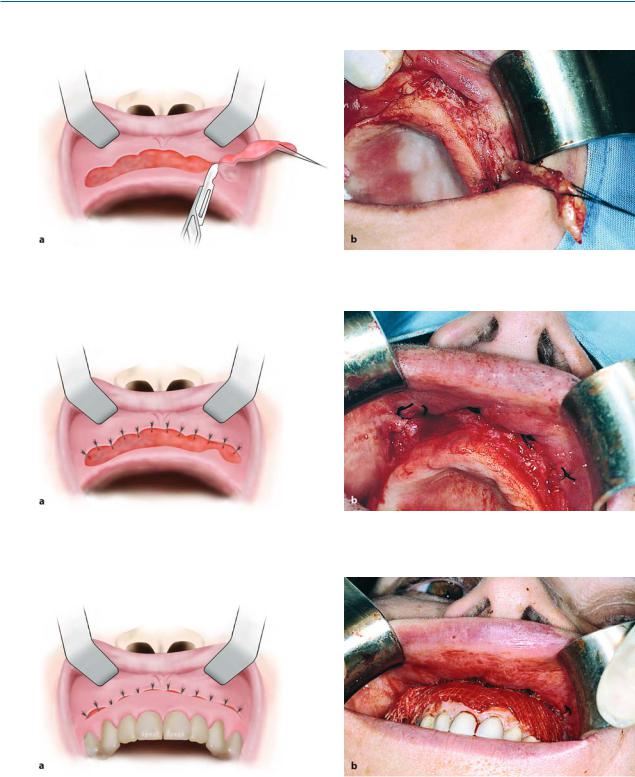
If the frenum is hypertrophic and there is a large space between the central incisors, the tissues found between and behind the central incisors are also removed (Fig. 10.79). Interrupted sutures are placed along the lateral margins of the wound in a linear direction, after the mucosa of the wound margins is undermined using scissors (Figs. 10.80–10.82).
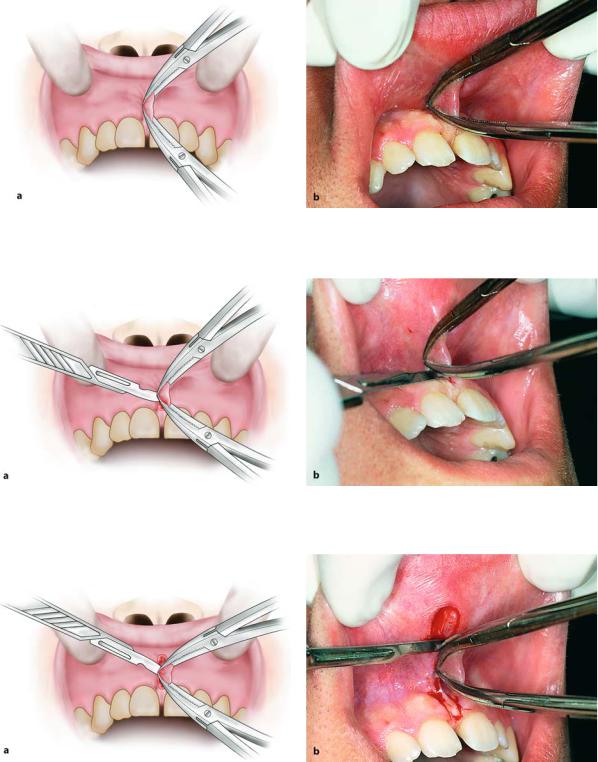
Fig. 10.74 a,b. Characteristic case of a maxillary labial frenum with a low gingival attachment. The orthodontist recommended its removal
Chapter 10 Preprosthetic Surgery |
263 |
Fig. 10.75 a,b. The superior and inferior margins of the frenum are grasped using curved mosquito hemostats. a Diagrammatic illustration. b Clinical photograph
Fig. 10.76 a, b. Initial step in excision of the frenum with a scalpel in contact with the posterior surface of the lower hemostat. a Diagrammatic illustration. b Clinical photograph
Fig. 10.77 a, b. Final step in excision of the frenum. Incision behind the upper hemostat is performed in a way similar to that shown in Fig. 10.76. a Diagrammatic illustration. b Clinical photograph

264 F. D. Fragiskos
Fig. 10.78 a,b. Surgical field after frenectomy. a Diagrammatic illustration. b Clinical photograph
Fig. 10.79 a, b. Removal of hypertrophic tissue found between and behind the central incisors. a Diagrammatic illustration. b Clinical photograph
Fig. 10.80 a,b. Undermining of mucosa of wound margins from underlying tissues. a Diagrammatic illustration. b Clinical photograph

Chapter 10 Preprosthetic Surgery |
265 |
Fig. 10.81 a,b. The first suture is placed at the middle of the wound to facilitate subsequent suturing. a Diagrammatic illustration. b Clinical photograph
Fig. 10.82 a,b. a Operation site after placement of sutures. b Postoperative clinical photograph 3 months later
10.2.1.2
Lingual Frenectomy
Removal of the lingual frenum is also a simple procedure, which may be performed with or without the help of a hemostat.
Technique Using Hemostat. After local anesthesia, the tongue is retracted upwards and posteriorly with a traction suture that is passed through the tip of the tongue. The frenum is then grasped approximately at the middle of the vertical length with a straight hemostat, which is parallel to the floor of the mouth
(Fig. 10.83). Using a scalpel the clasped portion of tissue is excised, first above the hemostat and then below (Figs. 10.84, 10.85). The wound margins are then undermined with scissors and interrupted sutures are placed (Figs. 10.86–10.88).
Technique Without the Aid of Hemostat. The lingual frenum may be removed with a scalpel without the aid of a hemostat. More specifically, after upward retraction of the tongue, the frenum is incised with converging incisions, first on the area of lingual attachment and then on the other side. After the frenum is loosened and the tongue is released, the tongue is retracted even further superiorly and posteriorly, to facilitate the removal of the rest of the frenum, which is still in place. After removal of the frenum, the wound margins are undermined and suturing follows, as outlined in the previous case (Figs. 10.89–10.93). Because the frenum is attached close to the deep lingual vein and the submandibular duct, careful attention must be given so that injury is avoided during the surgical procedure.
266F. D. Fragiskos
Steps in Frenectomy with Hemostat
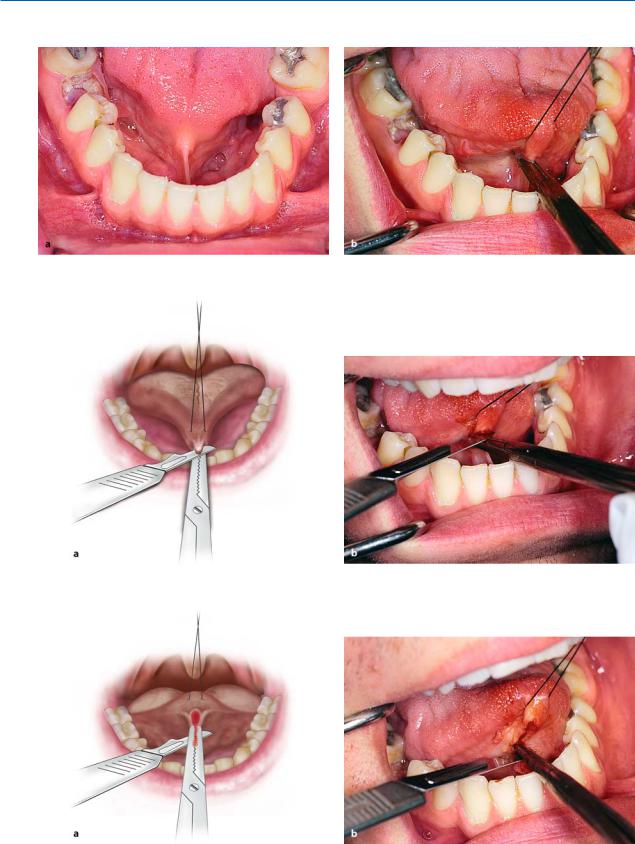
Fig. 10.83 a,b. a Lingual frenum (ankyloglossia) requiring surgical intervention. b Elevation of the tongue with the aid of a suture and retraction of the frenum with a straight hemostat, to facilitate removal
Fig. 10.84 a,b. First step in frenectomy. The scalpel is always in close contact with the upper surface of the hemostat. a Diagrammatic illustration. b Clinical photograph
Fig. 10.85 a,b. Second step in frenectomy, involving the portion beneath the hemostat. The procedure is similar to that shown in Fig. 10.84. a Diagrammatic illustration. b Clinical photograph
Chapter 10 Preprosthetic Surgery |
267 |
Fig. 10.86 a,b. Surgical field after removal of the frenum. a Diagrammatic illustration. b Clinical photograph
Fig. 10.87 a,b. Undermining the mucosa at wound margins from underlying tissues. a Diagrammatic illustration. b Clinical photograph
Fig. 10.88 a,b. Operation site after suturing. a Diagrammatic illustration. b Clinical photograph
268F. D. Fragiskos
Steps in Frenectomy without Hemostat
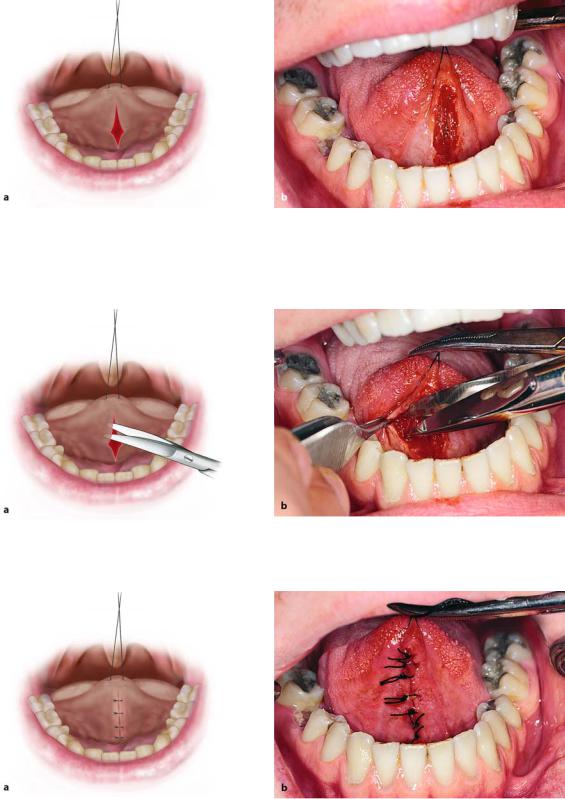
Fig. 10.89. Excision of the lingual frenum (case of ankyloglossia) using the technique without a hemostat
Fig. 10.91. Excision of the frenum with converging incisions towards the base of the tongue
Fig. 10.93. Operation site after the placement of sutures
Fig. 10.90. Elevation of the tongue with a suture placed at the tip of the tongue
Fig. 10.92. Undermining the wound margins with scissors
10.2.2
Denture-Induced Fibrous Hyperplasia
Fibrous hyperplasia of the mucosa (formerly known as epulis fissuratum or inflammatory hyperplasia) is usually due to chronic trauma of the mucosa of the mucolabial or mucobuccal fold, due to ill-fitting complete or partial dentures (Fig. 10.94). More specifically, the denture flanges injure this area, because they are very thin and longer than normal. The lesion may present during initial placement of the dentures, or after a period of time, when, due to resorption of the alveolar process, the anatomy of the region changes and the necessary adjustment of the prosthetic appliance is neglected. Treatment is surgical and consists of excision of the hyperplasia.

Chapter 10 Preprosthetic Surgery |
269 |
Surgical Technique. After local anesthesia, the lesion is grasped with surgical forceps and is gradually excised along the length of the lesion superficial to the underlying periosteum (Figs. 10.95, 10.96). After this procedure is complete, the portion of mucosa that has not been reflected, found at the margin of the lesion and which corresponds to the superior horizontal aspect of the incision, is sutured with the intact periosteum along its entire length, thus creating a void
(Fig. 10.97). Reattachment of the wound margins is therefore avoided, which would otherwise result in elimination of the depth of the mucolabial vestibule. After the surgical procedure, and after being lined with a tissue conditioner, the denture is inserted into the mouth and is continuously worn until the day the sutures are removed (Fig. 10.98). Almost the same procedure is performed for smaller lesions that are the result of ill-fitting dentures (Figs. 10.99–10.106).
Steps of Removal of Extensive Denture-Induced Fibrous Hyperplasia
Fig. 10.94 a,b. Extensive fibrous hyperplasia of the mucosa as a result of ill-fitting dentures. a Diagrammatic illustration. b Clinical photograph
Fig. 10.95 a,b. Removal of the lesion in segments with a scalpel. a Diagrammatic illustration. b Clinical photograph
270 F. D. Fragiskos
Fig. 10.96 a, b. Final step in the removal of hyperplasia. a Diagrammatic illustration. b Clinical photograph
Fig. 10.97 a, b. Suturing of the wound margins with periosteum that has not been reflected, which remains exposed, avoiding a decrease in the depth of the mucobuccal fold. a Diagrammatic illustration. b Clinical photograph
Fig. 10.98 a, b. Replacement of old denture, immediately after the end of the operation, retaining the depth of mucosa of the newly created sulcus. The internal surface of the
denture is lined with tissue conditioner. a Diagrammatic illustration. b Clinical photograph

Chapter 10 Preprosthetic Surgery |
271 |
Removal of Localized Denture-Induced Hyperplasia
Fig. 10.99. Localized fibrous hyperplasia of mucosa as a Fig. 10.100. Lesion of Fig. 10.99, after removal of denture result of ill-fitting denture
Fig. 10.101. Injection of local anesthetic peripherally |
Fig. 10.102. Gradual excision of hyperplasia with scalpel |
around the lesion |
and scissors |
Fig. 10.103. Surgical field after excision of lesion |
Fig. 10.104. Suturing of superior lip of incision with peri- |
|
osteum that has not been reflected, to avoid a decrease of the |
|
depth of the mucolabial fold |

272 F. D. Fragiskos
Fig. 10.105. Postoperative clinical photograph immediately after removal of sutures
10.2.3
Fibrous Hyperplastic Retromolar Tuberosity
Fibrous hyperplasia of the soft tissues of the alveolar process is reactive in nature, usually observed in the retromolar edentulous area of the maxilla and is the result of constant irritation during mastication. Clinically, bilateral asymptomatic symmetric lesions with a smooth surface are noted, which are elastic and firm during palpation. Size varies and sometimes the lesion may grow to be so big that it occupies all of the interarch space during occlusion, creating serious problems for construction of a partial or complete denture (Fig. 10.107). Treatment is surgical and aims to decrease the size of the fibrous connective tissue lesion, thus recontouring the alveolar process.
Fig. 10.106. Surgical specimen (hyperplasia) after excision
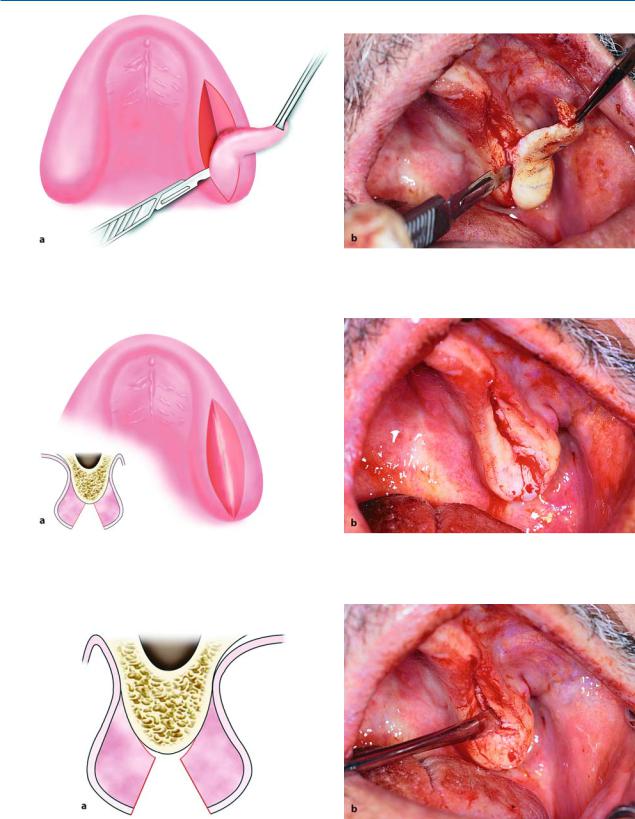
Surgical Technique. After administration of a local anesthetic, the portion of hyperplastic tissue to be excised is demarcated (Fig. 10.108). Two elliptic incisions are then made along the length of the fibrous hyperplasia, one buccally and the other palatally (Figs. 10.109,
10.110). The extent of divergence of the incisions depends on the size of the lesion. That is, the larger the diameter of the hyperplastic lesion, the more the incisions must diverge. The incisions begin at the site of formation of hyperplastic tissue, and are wedgeshaped, with the scalpel proceeding until it touches bone (Figs. 10.111, 10.112). The elongated wedgeshaped portion of the hyperplasia is then removed and the periosteum is reflected buccally and palatally, in order to readapt the wound margins (Fig. 10.113). Thereafter, the buccal and palatal parts are sutured at the midline of the alveolar ridge using a continuous suture (Figs. 10.114–10.116).
Fig. 10.107 a, b. Fibrous hyperplastic retromolar tuberosity of left maxilla. a Diagrammatic illustration. b Clinical photograph

Chapter 10 Preprosthetic Surgery |
273 |
Fig. 10.108 a, b. a Diagrammatic illustration and b clinical photograph showing demarcated segment of hyperplastic tissue to be removed
Fig. 10.109 a, b. Removal of lesion. a Diagrammatic illustration and b clinical photograph showing buccal incision
Fig. 10.110 a, b. Continuation of the incision of Fig. 10.109 towards the palatal side
274 F. D. Fragiskos
Fig. 10.111 a, b. Gradual excision of the lesion with a wedge-shaped incision reaching as far as the bone. a Diagrammatic illustration. b Clinical photograph
Fig. 10.112 a, b. Surgical field after removal of hyperplastic tissue. a Diagrammatic illustration. b Clinical photograph
Fig. 10.113 a, b. Reflection of tissues with periosteum, so that wound margins can be reapproximated and sutured

Chapter 10 Preprosthetic Surgery |
275 |
Fig. 10.114 a, b. Operation site after placement of sutures. a Diagrammatic illustration. b Clinical photograph
Fig. 10.115. Hyperplastic tissue segment after removal |
Fig. 10.116. Postoperative clinical photograph 6 months |
|
|
|
after the surgical procedure |
|
|
Clinically, these are multifocal hyperplastic nod- |
10.2.4 |
|
ules of the mucosa of the palate, between which food |
Papillary Hyperplasia of the Palate |
may accumulate, potentiating the inflammatory reac- |
|
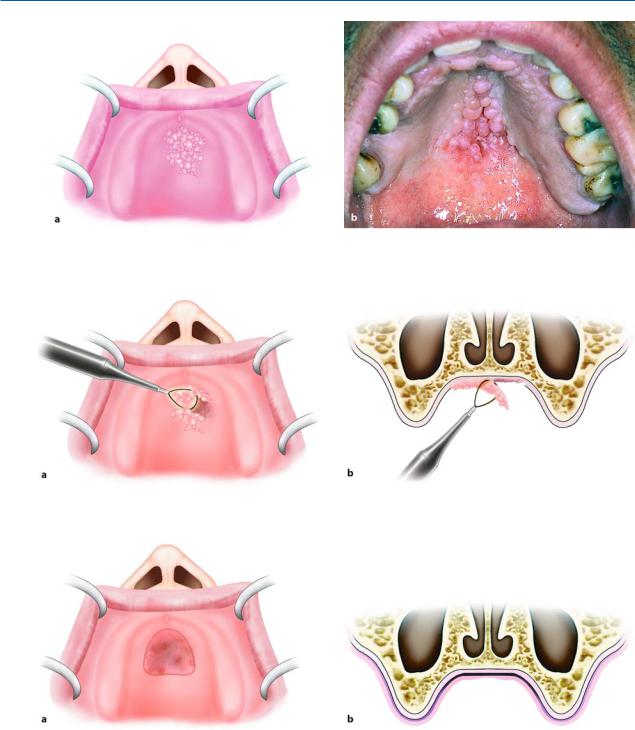
Papillary hyperplasia is a rare pathologic condition lo- |
tion. |
|
Treatment is surgical and consists of removal of the |
||
calized most often in the palate. It usually occurs in |
lesion with a scalpel or electrosurgical loop. |
|
edentulous patients who have been wearing dentures |
Surgical Technique. Excision of the papillary hyper- |
|
for a long time and is possibly due to inflammatory |
||
hyperplasia of the mucosa because of chronic local ir- |
plasia is performed with the instrument in constant |
|
ritation (Fig. 10.117 a). The lesion may present, to a |
contact with the superficial mucosa (curettage with |
|
limited extent, even in patients with dentition |
large surgical blade as far as the periosteum). An elec- |
|
(Fig. 10.117 b). In such a case, etiological factors in- |
trosurgical loop may also be used (Fig. 10.118), which |
|
clude mechanical and thermal irritation from foods, |
is very effective in such cases. The traumatized area is |
|
smoking, etc. |
covered with a surgical dressing and healing is achieved |
|
|
|
by secondary intention (Fig. 10.119). |
276 F. D. Fragiskos
Fig. 10.117 a, b. Papillary hyperplasia of the palate. a Diagrammatic illustration of the lesion in an edentulous patient. b Clinical photograph in a patient with full dentition
Fig. 10.118 a, b. Diagrammatic illustrations showing removal of the lesion with an electrosurgical loop
Fig. 10.119 a, b. Diagrammatic illustrations showing the surgical field after removal of the lesion

Chapter 10 Preprosthetic Surgery |
277 |
10.2.5
Gingival Fibromatosis
This is a benign condition, which is characterized by slow progressive swelling of the gingivae proper (attached gingivae) and alveolar mucosa (loose gingivae). The lesion may be generalized or localized and is due to hereditary or acquired causes.
Clinically, gross hyperplasia of the gingivae is observed, which may partially or completely cover the crowns of the teeth, depending on the case. The surface of the gingivae is lobular, reddish, and firm to palpation, while the inflammation and bone resorption vary (Figs. 10.120, 10.121).
Treatment is surgical and consists of segmental excision of the gingivae.
Surgical Technique. After administration of a local anesthetic, the teeth presenting excessive mobility are removed. An incision is then made on the alveolar ridge and the hyperplastic gingivae are reflected buccally and lingually (Fig. 10.122). Excision of the lesion is performed in segments with beveling and is done very carefully, so that the mental and lingual nerves are not injured (Figs. 10.123, 10.124). The alveolar ridge is then smoothed and, after the wound margins are reapproximated, interrupted sutures are placed (Figs. 10.125–10.127).
Fig. 10.120. Radiograph depicting thinning of the roots of mandibular molars and bone resorption in the area
Fig. 10.121. Clinical photograph of case shown in Fig. 10.120, showing gross lobular swelling of the gingivae
Fig. 10.122. Incision along the alveolar ridge and reflection of buccal and lingual gingivae
Fig. 10.123. Gradual removal of hyperplastic gingivae, beveling in segments