360 G. Perdikaris, A. Pefanis, E. Giamarellou
antibiotic prophylaxis) did not show a decreased incidence in the group that was administered an antibiotic, we cannot recommend their administration. Some studies showed that the prophylactic administration of antibiotics resulted in fewer, noninfectious complications, such as trismus, pain, edema, and fibrinolytic alveolitis (dry socket). Even so, some of these studies presented methodological planning problems. Two recent reviews do not recommend routine prophylactic administration of antibiotics for surgical extraction of the impacted third molar, concluding that their administration is justified only in very difficult cases, for example when impaction is deep and a large amount of bone has to be removed. Also, according to the recommendations of the British Society for Antimicrobial Chemotherapy (1992) administration of prophylaxis is not recommended for this surgical procedure.
To conclude, it must be emphasized that the administration of antibiotics for a period greater than 24–
48 h after the operation is not considered prophylaxis but therapy. Indications for therapy are limited and include: (a) the presence of edema with pain or sensitivity that suggests cellulitis or an abscess that must absolutely be drained, (b) presence of trismus, unless it is secondary to postoperative edema, hematoma, trauma, (c) presence of purulent exudate, unless the cause was removed and the focal site of infection is far from the airway passages, (d) no improvement of symptoms
48 h later or worsening 36 h or more after surgical procedure, and (e) tachycardia (>100 beats per min) and fever (>38 °C). Fever is not necessarily a symptom of infection, especially in elderly people in whom severe infection may occur without fever.
In conclusion and according to recent data, prophylaxis with antibiotics is recommended for few dental procedures. In these limited cases the antibiotic must be administered shortly before the operation. A second dose is recommended only in the case of extensive and prolonged surgery.
16.3 Osteomyelitis
Osteomyelitis is a rare complication of odontogenic infections. In most cases it is the result of spread of infection from a dentoalveolar or periodontal abscess, or from the paranasal sinuses, by way of continuity through tissue spaces and planes. It occasionally occurs as a complication of jaw fractures, or as a result of abusive manipulations during surgical procedures. It is classified as acute or chronic osteomyelitis.
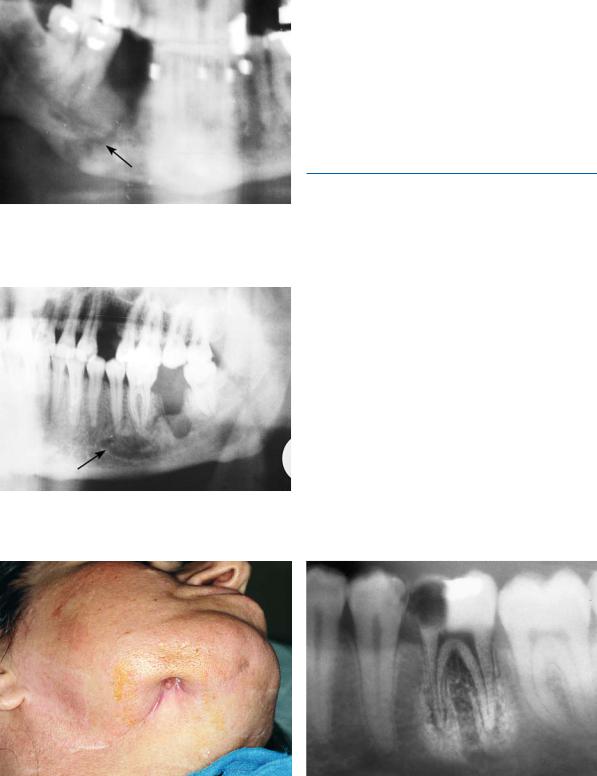
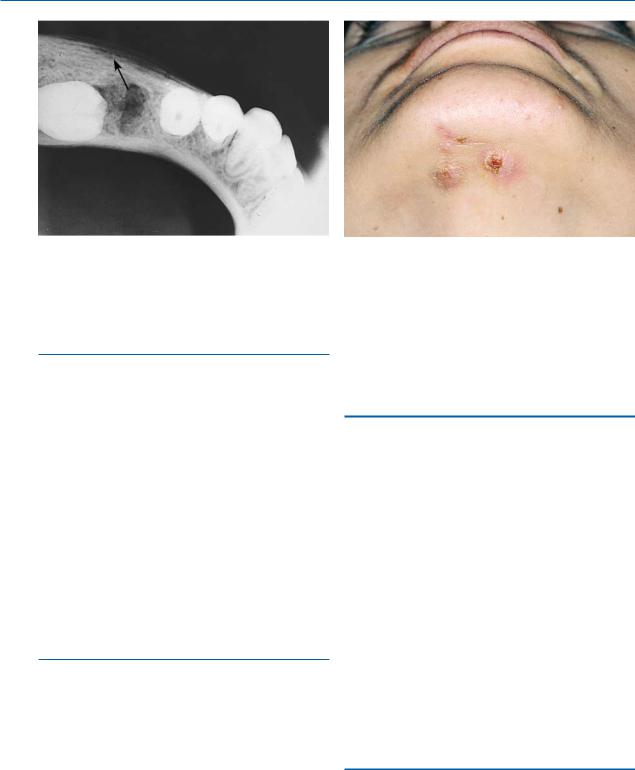
In the acute form, which, though rarely, may also be of hematogenous origin, the infection begins in the medullary cavity of the bone. The resulting increase of intrabony pressure leads to a decreased blood supply and spread of the infection, by way of the Haversian canals, to the cortical bone and periosteum. This aggravates the ischemia, resulting in necrosis of the bone. Predisposing factors include compromised host defenses due to compromised local blood supply (Paget’s disease, radiotherapy, bone malignancy, etc.), or systemic disease (e.g., alcoholism, diabetes mellitus, leukemia, AIDS, etc.), and infection from microorganisms with great virulence. In such cases even a periapical abscess may be implicated in osteomyelitis. The mandible, due to decreased vascularity, is involved 6 times more often than the maxilla. The main pathogens are streptococci, Klebsiella spp., Bacteroides spp., and other anaerobic bacteria. Piercing, deep, and constant pain predominates in the clinical presentation in adults, while low or moderate fever, cellulitis, lymphadenitis, or even trismus may also be noted. In the mandible, paresthesia or dysesthesia of the lower lip may accompany the disease. When the disease spreads to the periosteum and the surrounding soft tissues, a firm painful edema of the region is observed, while the tooth becomes loose and there is discharge of pus from the periodontium. Radiographic examination reveals osteolytic or radiolucent regions (Figs. 16.1, 16.2), which sometimes surround a portion of dense bone (sequestrum). Therapy entails combined surgical (incision, drainage, extraction of the tooth, and removal of sequestrum) and pharmaceutical treatment with antibiotics. Antibiotics must be administered intravenously, in large doses, for at least 3–4 days after the fever ceases. Treatment may then continue orally for another 2–4 weeks, depending on the extent of the disease, the causative pathogen, and the clinical response. The antibiotic of choice is penicillin (3 =106 units every 4 hours, i.v.), and in the case of allergy to penicillin, clindamycin is administered (600 mg every 6 h, i.v.). If staphylococcus or another
“difficult” to treat microorganism develops, consultation with an infectious diseases specialist is recommended. In the case of fracture of the mandible, which has occurred over 48 h previously, the possibility of osteomyelitis is great. The patient should be administered antibiotic therapy intravenously as soon as possible, particularly in cases of compound fractures of the mandible.
Chronic osteomyelitis is characterized by a clinical course lasting over a month. It may occur after the acute phase, or it may be a complication of odontogenic infection without a preceding acute phase. The clinical