

Chapter 6
Surgical extraction is the method by which a tooth is removed from its socket, after creating a flap and removing part of the bone that surrounds the tooth. This technique is relatively simple and within a general practitioner’s scope if the basic principles of the surgical technique are followed.
6.1 Indications
The main indications for performing a surgical extraction are:
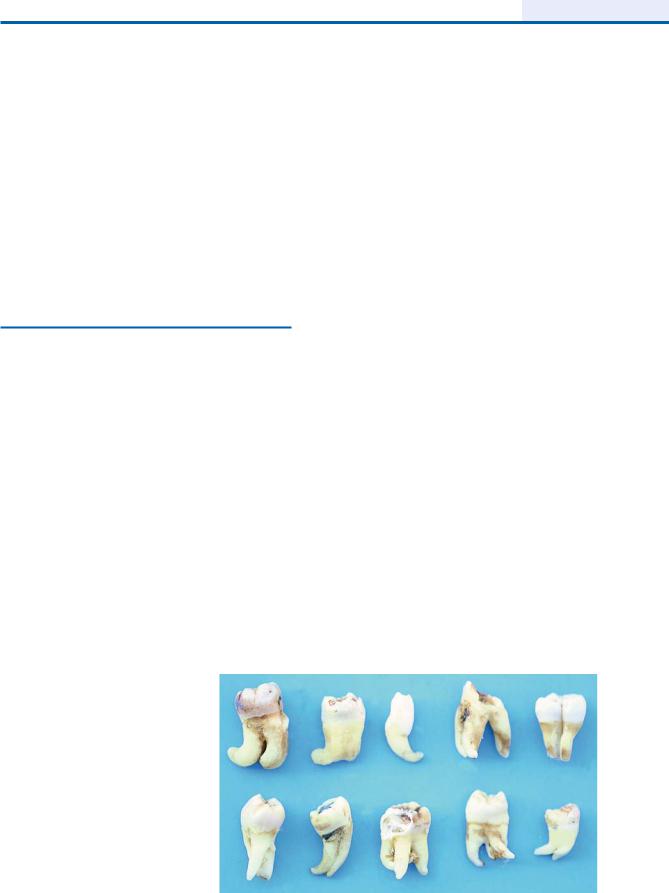
ΟTeeth of the maxilla or mandible that present unusual root morphology (Fig. 6.1). In such cases, a surgical extraction is performed preventively, because their removal is impossible with the simple technique without complications arising (e.g., root breaking, fracture of alveolar bone, etc.).
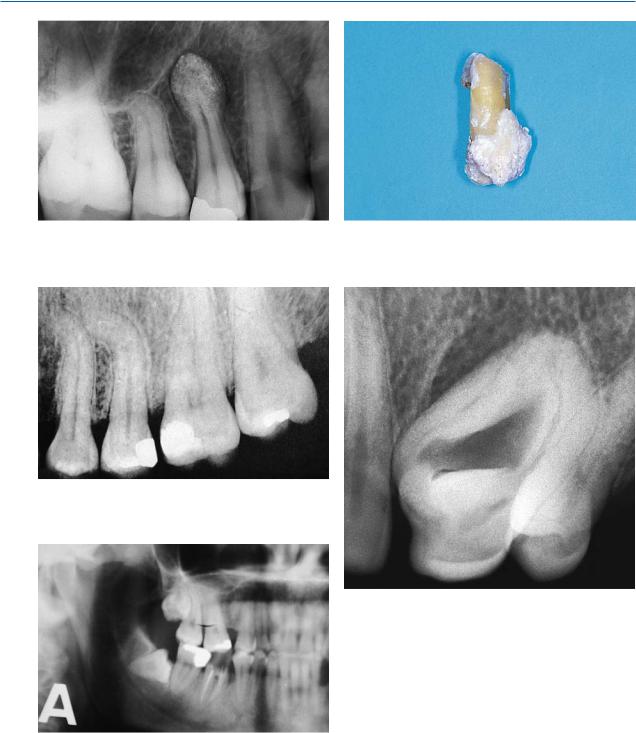
ΟTeeth with hypercementosis of root and root tip, presenting large bulbous roots (Figs. 6.2, 6.3).
ΟTeeth with dilaceration of root tips (Fig. 6.4).
ΟTeeth with ankylosed roots or with abnormalities, e.g., dens in dente (Fig. 6.5).
ΟImpacted and semi-impacted teeth (Fig. 6.6). The extraction of these teeth is accomplished employing a surgical technique, depending on the type and
Fig. 6.1. Teeth with unusual root morphology. Surgical technique is indicated for removal
Surgical Tooth Extraction |
6 |
|
|
F. D. Fragiskos |
|
|
|
localization of the impacted or semi-impacted tooth
(see Chap. 7).
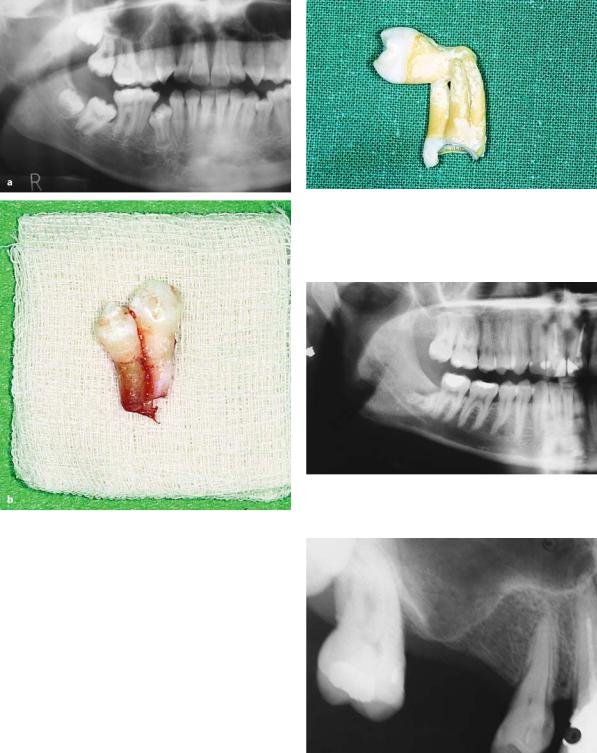
ΟTeeth fused with an adjacent tooth (Fig. 6.7a, b) or teeth fused with an adjacent tooth in the apical area (Fig. 6.8). If extraction were to be attempted using the simple technique in these unusual cases, then part of the alveolar process could be fractured or removed together with the teeth.
ΟBroken root tips that have remained in the alveolar bone (Fig. 6.9) and are involved in osteolytic lesions, or are in such a position that, in the case of denture placement, they could create problems in the future.
ΟMaxillary posterior teeth, whose roots are included in the maxillary sinus (Fig. 6.10). When the maxillary sinus extends as far as the alveolar ridge, the bone found in the posterior area of the maxilla is also weakened. This increases the risk of fracture of the maxillary tuberosity if the extraction involves a firmly anchored tooth (molar), because with the simple technique great forces are generated during its removal.
ΟRoots of teeth found below the gumline, when their removal is impossible any other way (Figs. 6.11,
6.12).
ΟRoots with periapical lesions, whose entire removal through the tooth socket would not be possible with curettage alone (Figs. 6.13–6.15).
96 F. D. Fragiskos
Fig. 6.2. Radiograph showing maxillary premolar with |
Fig. 6.3. Hypercementosis of root of mandibular second |
hypercementosis at root tip |
premolar |
Fig. 6.4. Root tips of first and second premolar, with nearly right-angle curvature compared to long axis of teeth
Fig. 6.5. Dens in dente of maxillary left canine
Fig. 6.6. Semi-impacted mandibular third molar. Surgical technique is indicated for removal
Chapter 6 Surgical Tooth Extraction |
97 |
Fig. 6.7 a,b. a Panoramic radiograph, showing fusion of two mandibular premolars. b The same fused teeth after their removal
ΟDeciduous molars whose roots embrace the crown of the subjacent premolar. If the simple extraction technique were to be attempted, there is a great risk of concurrent luxation of the premolar (Fig. 6.16).
ΟPosterior teeth with supraeruption. It is well known that when the antagonist is missing, these teeth present supraeruption to a great degree, which is accompanied by the dragging down of the alveolar process. As such, the extraction must be carried out using the surgical technique with concurrent recontouring of the alveolar process of the area (see Chap. 10).
Fig. 6.8. Maxillary second molar for which the surgical technique is indicated for removal. During the procedure the third molar would be removed as well, due to fusion of the two teeth in the apical area
Fig. 6.9. Radiograph showing root tips of mandibular third molar, which are close to the mandibular canal
Fig. 6.10. Pneumatization of the maxillary sinus into the alveolar process of the edentulous area corresponding to the maxillary first molar
98 F. D. Fragiskos
Fig. 6.11. Radiograph showing the mesial root of the mandibular first molar, entirely covered by bone
Fig. 6.13. Radiograph showing roots with large periapical lesions. Their removal is only possible with the surgical technique
Fig. 6.12. Roots of maxillary and mandibular molars completely covered by bone
Fig. 6.14. Root of mandibular left first premolar, with extensive periapical lesion
Fig. 6.15. Root of 44 displaced into pathologic lesion, after unsuccessful removal attempt
Fig. 6.16. Deciduous mandibular molar, whose roots embrace the crown of the succedaneous premolar. Risk of concurrent luxation with the simple extraction technique