


114 F. D. Fragiskos
Fig. 6.65 a, b. a Small portion of the buccal plate is removed and a groove created at the surface of the root, at a 45° angle to the long axis of the tooth. b Placement of the double-angled elevator in the purchase point of the root for luxation
Fig. 6.66 a, b. a Groove created between the root and buccal bone for elevator placement. b Luxation of the root with angled Seldin elevator
6.6
Surgical Extraction of Root Tips
When a root tip is fractured deep in the socket and is impossible to remove with simple luxation, its removal may be accomplished using one of the aforementioned techniques for removal of roots, depending on the situation.
The dentist must pay particular attention when removing root tips that have been dislodged towards the maxillary sinus.
When a root or root tip of a posterior maxillary tooth is fractured and displaced into the maxillary sinus during the luxation attempt, it is a serious complication and must be dealt with as soon as possible. In order to avoid such a possibility, before any extraction of a posterior maxillary tooth, radiographs must be examined carefully to determine how close the root tips are to the maxillary sinus.
This close proximity is usually observed when the maxillary sinus is pneumatized into the alveolar process between the root tips of molars and especially when there are periapical lesions that are in contact with the lower surface of the maxillary sinus. In cases
Chapter 6 Surgical Tooth Extraction |
115 |
such as these, if a root tip is fractured, it may be displaced into the maxillary sinus fairly easily if movements during the luxation attempt are not gentle and if special narrow instruments are not used.
6.6.1
Surgical Technique
If the root tip has actually been displaced into the maxillary sinus, the patient is informed at once about the situation and a new appointment is scheduled so that removal of the root tip and closure of the oroantral communication are accomplished in the same session. If the dentist doubts his or her ability to treat the complication, then the patient should be referred to a special surgeon. The procedure in this case is as fol-
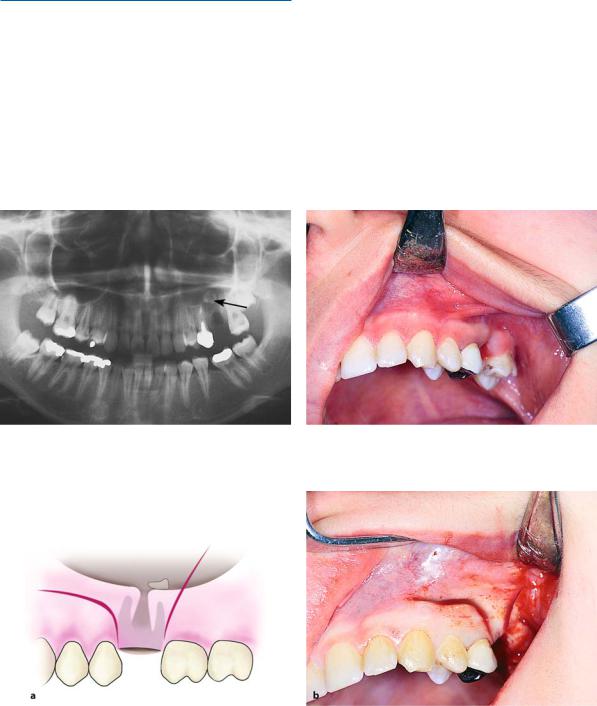
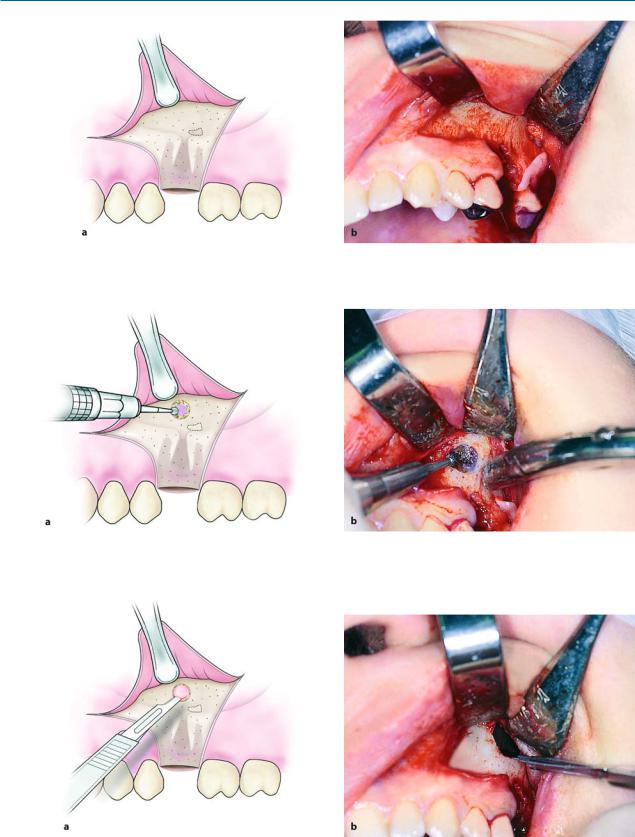
lows. After radiographic confirmation and precise localization of the root tip in the maxillary sinus (Figs. 6.67, 6.68), a straight incision is made, which begins at the canine and ends in a trapezoidal shape, including the postextraction socket (Fig. 6.69). After reflection of the flap, access to the maxillary sinus is accomplished by opening a window at the buccal bone
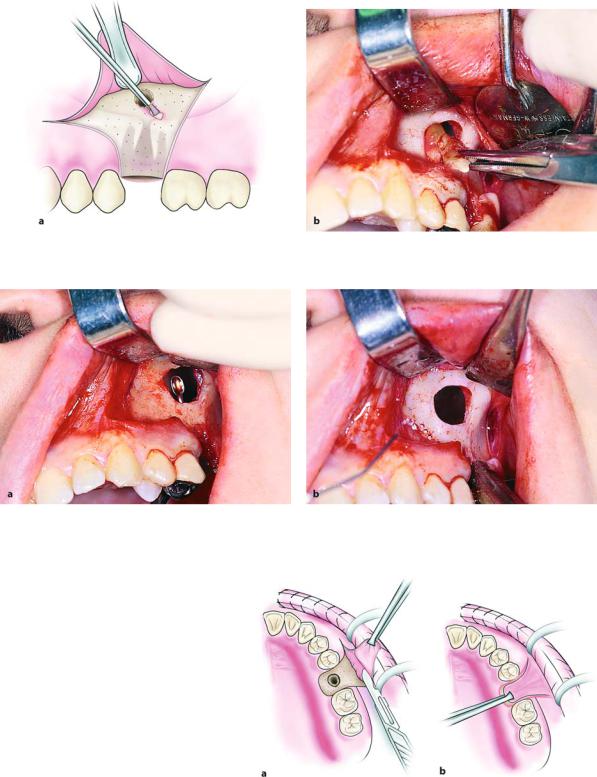
(Figs. 6.70, 6.71). The mucosa of the maxillary sinus is then incised using a scalpel, and after the root tip is localized following inspection of the area, the root tip is removed using the suction or anatomic forceps (Figs. 6.72, 6.73). If there is granulation tissue in the area of the fistula, it is removed using a periapical curette through the aperture in the maxillary sinus and through the socket itself (Fig. 6.74). Immediately after removal of the root tip, closure of the oroantral communication follows. More specifically, the existing
Fig. 6.67. Panoramic radiograph showing the root tip of |
Fig. 6.68. Clinical photograph of the case shown in |
the first molar displaced into the maxillary sinus |
Fig. 6.67 |
Fig. 6.69 a, b. Surgical procedure for removal of a root |
creation of the appropriate flap. a Diagrammatic illustra- |
tip from the maxillary sinus and closure of the oroantral |
tion. b Clinical photograph |
communication in the same surgical session. Incision for |
|
116 F. D. Fragiskos
Fig. 6.70 a,b. Reflection of flap and removal of bone to allow access to the maxillary sinus. a Diagrammatic illustration. b Clinical photograph
Fig. 6.71 a, b. Access to the maxillary sinus above the postextraction socket. The antral mucosa is revealed through the created aperture. a Diagrammatic illustration. b Clinical photograph
Fig. 6.72 a, b. Maxillary sinus opened with incision in mucosa. a Diagrammatic illustration. b Clinical photograph
Chapter 6 Surgical Tooth Extraction |
117 |
Fig. 6.73 a, b. Removal of root tip from the maxillary sinus together with a portion of mucosa found above and around the orifice of the communication. a Diagrammatic illustration. b Clinical photograph
Fig. 6.74 a, b. a Periapical curette used to examine if inflammatory tissue has been removed from the area through the socket. b Surgical field at the end of the operation
Fig. 6.75 a, b. a Horizontal incision of the periosteum at the base and center of the flap
to ensure elasticity, so that it is adequate to cover the fistula. b Examination of the flap’s elasticity with traction towards the suturing position
trapezoidal flap is lengthened with a horizontal incision of the periosteum at the middle and the base of the flap, so that the flap is big enough to cover the fis-
tula (Fig. 6.75 a, b). The bone edges of the wound are then smoothed and the flap is repositioned and sutured with the palatal soft tissues, which have already