


Chapter 8 Perioperative and Postoperative Complications |
195 |
Treatment. No particular therapy is indicated for neurapraxia or axonotmesis, unless there is a root tip or other foreign body compressing the nerve, in which case it must be removed. Treatment is usually palliative, including the administration of analgesics in painful situations, and multi-vitamin supplements of the vitamin B complex to restore sensation more rapidly. Damage to the nerve as a result of neurotmesis must be treated as soon as possible; often, a graft must replace the injured nerve segments or the severed segments must be sutured.
8.2
Postoperative Complications
8.2.1 Trismus
Trismus usually occurs in cases of extraction of mandibular third molars, and is characterized by a restriction of the mouth opening due to spasm of the masticatory muscles (Fig. 8.44). This spasm may be the result of injury of the medial pterygoid muscle caused by a needle (repeated injections during inferior alveolar nerve block) or by trauma of the surgical field, especially when difficult lengthy surgical procedures are performed. Other causative factors are inflammation of the postextraction wound, hematoma, and postoperative edema.
Treatment. The management of trismus depends on the cause. Most cases do not require any particular therapy. When acute inflammation or hematoma is the cause of trismus, hot mouth rinses are recommended initially, and then broad-spectrum antibiotics are administered. Other supplementary therapeutic measures include:
ΟHeat therapy, i.e., hot compresses are placed extraorally for approximately 20 min every hour until symptoms subside
ΟGentle massage of the temporomandibular joint area
ΟAdministration of analgesics, anti-inflammatory and muscle relaxant medication
ΟPhysiotherapy lasting 3–5 min every 3–4 h, which includes movements of opening and closing the mouth, as well as lateral movements, aimed at increasing the extent of mouth opening (Fig. 8.45)
ΟAdministration of sedatives [bromazepam (Lexotanil): 1.5–3 mg, twice daily], for management of stress, which worsens while trismus persists, leading to an increase of muscle spasm in the area
Fig. 8.44. Reduced aperture of the mouth due to trismus
Fig. 8.45. Attempt to open mouth with physiotherapy, in a case of trismus
8.2.2 Hematoma
This is a quite frequent postoperative complication due to prolonged capillary hemorrhage (Fig. 8.46), when the correct measures for control of bleeding are not taken (ligation of small vessels, etc.). In this case blood accumulates inside the tissues, without any escape from the closed wound or tightly sutured flaps under pressure. Depending on the operation, the hematoma may be submucosal, subperiosteal, intramuscular or fascial. As for patients with hemorrhagic diatheses, hematomas formed in the palatopharyngeal arches are considered most dangerous of all.
Treatment. If a hematoma is formed during the first few hours after the surgical procedure, therapeutic management consists of placing cold packs extraorally during the first 24 h, and then heat therapy to help it to subside more rapidly. Some people recommend the administration of antibiotics to avoid suppuration of the hematoma, and analgesics for pain relief.

196 F. D. Fragiskos
Fig. 8.46. Hematoma as a result of surgical extraction |
Fig. 8.47. Diffuse ecchymosis after surgical removal of the |
|
root of a mandibular premolar. This may be the result of |
|
excessive retraction of the flap using retractors |
Fig. 8.48. Edema as a result of a difficult surgical procedure to remove an impacted mandibular third molar. The patient did not present with fever, just a mild trismus
8.2.3 Ecchymosis
Fig. 8.49. Edema of the lower eyelid with a skin hue ranging from very red to cyanotic, as a result of the surgical removal of an ankylosed maxillary canine. Manipulations and pressure exerted by retractors often lead to such clinical images
8.2.4 Edema
In certain cases, after the surgical procedure, ecchymosis may develop on the patient’s skin, which presents as friable capillaries and decreased tissue tone.
Other than the generalized trauma of the area, it may be the result of damage during flap retraction with various retractors (Fig. 8.47). In order to avoid such a complication, retractors must be handled gently, especially in the region of the mental foramen, zygomaticoalveolar crest, and canine eminence.
Treatment. No particular treatment is required. The patient should be informed that it is not a serious situation and that ecchymoses gradually subside within a few days, changing color in the process.
Edema is a complication secondary to soft tissue trauma, up to a point. It is the result of extravasation of fluid by the traumatized tissues because of destruction or obstruction of lymph vessels, resulting in the cessation of drainage of lymph, which accumulates in the tissues. Swelling reaches a maximum within 48–72 h after the surgical procedure and begins to subside on the third or fourth day postoperatively. Clinically, the edema is characterized by smooth, pale, and taut skin
(Fig. 8.48). When swelling is due to inflammation, the skin presents with redness, because of the local hyperemia (see Chap. 9). Depending on the amount of tissue injury in the area, the edema ranges from small to moderate and, rarely, severe. Sometimes, when the
Chapter 8 Perioperative and Postoperative Complications |
197 |
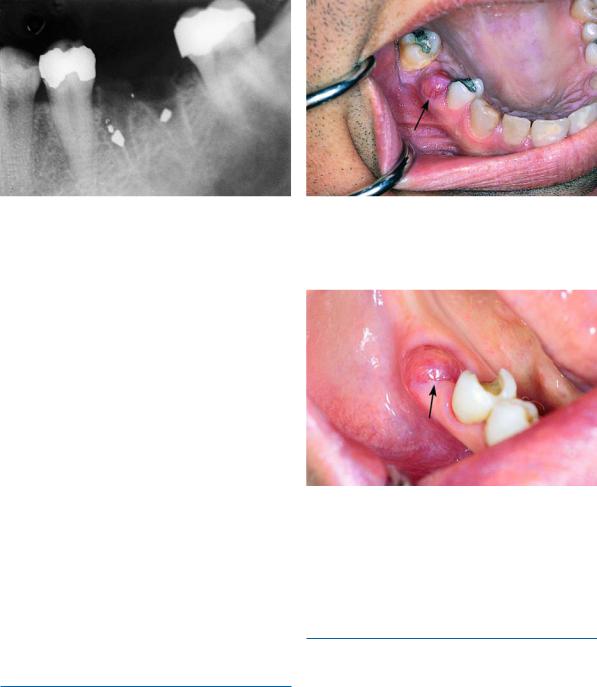
Fig. 8.50. Periapical radiograph of the region of the mandibular first molar, showing amalgam remnants inside the alveolar cavity, responsible for the development of a postextraction granuloma
surgical procedure is performed in the maxilla, the edema may extend as far as the lower eyelid, either because the tissues in this area are especially loose (Fig. 8.49), or because the patient may have a bleeding disorder (latent purpura, etc.). In such cases, the skin hue is cyanotic.
Treatment. A small-sized edema does not require any therapeutic management. For preventive reasons, cold packs should be applied locally immediately after surgery. They should be placed for 10–15 min every half hour, for the following 4–6 h. When the edema is severe and especially if it does not subside, it must be treated carefully, because an edema present for a prolonged period may lead to fibrosis and development of symphyses. In this case the administration of proteolytic or fibrinolytic medication is indicated, and if the edema is secondary to inflammation, then broadspectrum antibiotics are also prescribed. If the edema spreads towards the pharyngomaxillary region (danger of asphyxia), then intravenous administration of
250–500 mg hydrocortisone is indicated, which has a rapid action with excellent results.
8.2.5
Postextraction Granuloma
This complication occurs 4–5 days after the extraction of the tooth and is the result of the presence of a foreign body in the alveolus, e.g., amalgam remnants, bone chips, small tooth fragments, calculus, etc. (Fig. 8.50). Foreign bodies irritate the area, so that postextraction healing ceases and there is suppuration of the wound (Figs. 8.51, 8.52).
Fig. 8.51. Clinical photograph of a postextraction granuloma shown in Fig. 8.50
Fig. 8.52. Postextraction granuloma in the region of the left mandibular first molar
Treatment. This complication is treated with debridement of the alveolus and removal of every causative agent.
8.2.6
Painful Postextraction Socket
This is a common complication, which occurs immediately after the anesthetic wears off. It occurs mainly at the postextraction wound of mandibular posterior teeth, although maxillary posterior teeth may also be involved, due to the anatomy of the bone (dense), where sharp bony spicules are easily created, especially if the extractions are difficult and are performed with awkward manipulations. The uneven bone edges injure the soft tissues of the postextraction socket, resulting in severe pain and inflammation at the extrac-
198 F. D. Fragiskos
Fig. 8.53. Clinical photograph of a painful postextraction socket with irregular sharp bone edges, which cause injury to soft tissues covering the bone
Fig. 8.54. Periapical radiograph showing sharp spicules of alveolar bone, which remained after the extraction of a tooth
tion site (Figs. 8.53–8.56). In this case, the alveolus is filled with a blood clot that becomes organized for postextraction healing, but not for development of epithelium that will cover the wound.
Treatment. This complication is treated with smoothing of the bone margins of the wound, especially the intraradicular bone (Fig. 8.57). In addition to giving the patient analgesics, gauze impregnated with eugenol should be placed over the wound margins for 36–48 h.
Fig. 8.55. Clinical photograph of case shown in Fig. 8.54, showing sharp bone edges that injure the soft tissues of the postextraction socket
Fig. 8.56 a,b. Painful postextraction socket that is the result of a bone edge projecting from intraradicular bone. a Radiograph and b clinical photograph

Chapter 8 Perioperative and Postoperative Complications |
199 |
Fig. 8.57 a,b. Treatment of the case shown in Fig. 8.56. Removal of portion of intraradicular bone with bone rongeur
8.2.7
Fibrinolytic Alveolitis (Dry Socket)
This postoperative complication appears 2–3 days after the extraction. During this period, the blood clot disintegrates and is dislodged, resulting in delayed healing and necrosis of the bone surface of the socket (Fig. 8.58). This disturbance is termed fibrinolytic alveolitis and is characterized by an empty socket, fetid breath odor, a bad taste in the mouth, denuded bone walls, and severe pain that radiates to other areas of the head.
As for the etiology and pathogenesis of dry socket, various factors have been cited, some of which include dense and sclerotic bone surrounding the tooth, infection during or after the extraction, injury of the alveolus, and infiltration anesthesia.
Treatment. This type of complication is treated by gently irrigating the socket with warm saline solution, and placing gauze impregnated with eugenol, which is replaced approximately every 24 h, until the pain subsides. Also, gauze soaked in zinc-oxide/eugenol may be used, which remains inside the alveolus for 5 days; alternatively iodoform gauze or enzymes are applied locally. Recent studies have shown Matthews’ (1982) and Mitchell’s (1986) techniques to be very effective.
They used dextranomer granules (Debrisan) and collagen paste (Formula K) without observing a foreign body reaction like that observed with the zinc-oxide/ eugenol mix. With this palliative treatment, the pain gradually subsides, and the patient is given instructions to avoid mastication on the affected side while good oral hygiene is emphasized.
Fig. 8.58. Clinical photograph of fibrinolytic alveolitis (dry socket) in the region of the maxillary second molar
8.2.8
Infection of Wound
Infection of the wound is a complication that may present and spread not only to the superficial surgical wound, but also to the depth and extent of the tissues involved in the surgical manipulations. Infection of the wound may be caused by:
ΟThe use of infected instruments and disposable materials during the surgical procedure.
ΟA septic substrate over which the surgical procedure is performed.
ΟDefective bone substrate secondary to diseases of the skeletal system (osteopetrosis), and radiotherapy of the jaw and facial area.