


60 F. D. Fragiskos
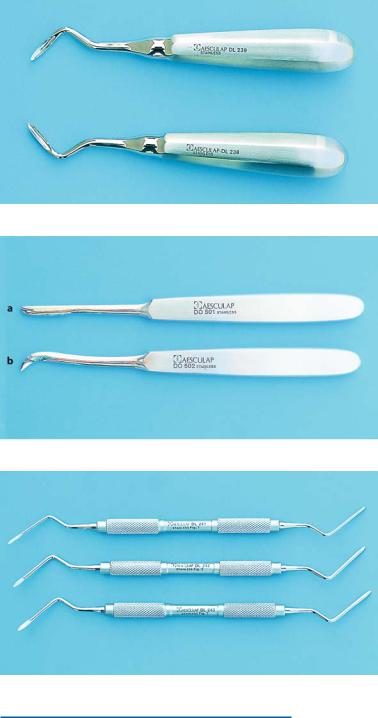
Mandibular Root Tip Forceps. The handles of the root tip forceps are straight, while the beaks are curved at a right angle. Their ends are very narrow and meet at the tip when the forceps are closed (Fig. 4.46).
4.20 Elevators
The elevator is the second most important instrument (after the extraction forceps) with which tooth extraction is achieved or aided. It is composed of three parts: the handle, the shank, and the blade. The shape of blade differs for each elevator type, and each is used as the need dictates. There are three main types of elevators used today in oral surgery: the straight elevator, the pair of elevators with T-shaped or crossbar handles, and the pair of double-angled elevators.
Straight Elevator. This is the most commonly used type of elevator for the removal of teeth and roots, in both the upper and lower jaws (Figs. 4.47, 4.48). As already mentioned, the elevator’s components are the handle, shank, and blade. The handle is pear-shaped, and big enough to be held comfortably in the hand for the surgeon to apply pressure to the tooth to be luxated. The shank is narrow and long and connects the handle to the blade. The blade has two surfaces: a convex and a concave one. The concave surface is placed buccally, either perpendicular to the tooth or at an angle, and always in contact with the tooth to be luxated. The elevator is held in the dominant hand, and the index finger is placed along the blade almost reaching its end. The end of the blade is left exposed and is seated between the socket and the tooth to be luxated.
Fig. 4.46. Mandibular root tip forceps
Pair of Elevators with T-shaped or Crossbar Handles.
This type of elevator (Fig. 4.49) is used only in the lower jaw for removal of a root of a molar, after the other root has already been removed with the straight elevator. Each of these elevators is composed of the handle, shank, and blade. The shank is connected to the middle of the handle, giving the elevator a T-shaped appearance, while the connection of the shank to the blade is angled, and the blade end is sharp-tipped. The blades on this pair of elevators face in opposite directions, and the appropriate one is used according to the root that has to be removed. One elevator is used to remove the mesial root, and the other for the distal root, for each side of the lower jaw. Angled Seldin elevators are a variation of the elevators with T-shaped handles (Fig. 4.50).
In certain cases, the T-shaped elevator may be used to remove a whole third molar of the lower jaw. The tip of the elevator is placed into the root bifurcation buccal to the tooth, using the external oblique ridge as a fulcrum.
Pair of Double-Angled Elevators. Double-angled elevators are mainly used to remove root tips in both jaws. They are also very useful instruments for the extraction of impacted third molars of the upper jaw (Fig. 4.51). Their handle is similar to that of the straight elevator. The shank has a double angle, so that the instrument may enter the socket, and the two elevators face in opposite directions. The blade has a convex and concave surface, ending in a sharp point. There are also double-angled elevators with narrow blades and very sharp ends, which may easily remove small broken root tips.

Chapter 4 Equipment, Instruments, and Materials |
61 |
Fig. 4.47. Straight Bein elevator
Fig. 4.48. Straight White elevator with slightly curved blade, suitable for extracting posterior maxillary teeth
Fig. 4.49. Pair of elevators with crossbar or T-shaped handles
Fig. 4.50. Pair of angled Seldin elevators suitable for extracting roots in the mandible
62 |
F. D. Fragiskos |
Fig. 4.51. Pair of double-angled elevators
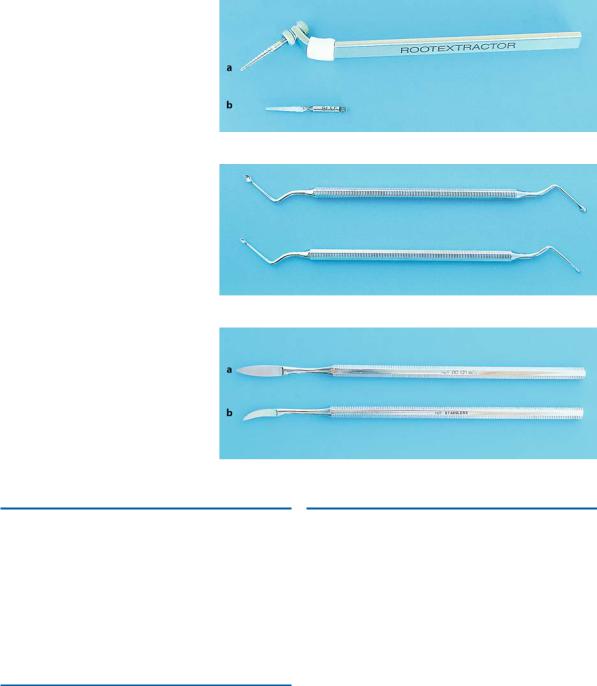
Fig. 4.52 a, b. Chompret elevators; a straight, and b curved
4.21
Other Types of Elevators
Straight Chompret Elevator. The narrow blade of this instrument means that this type of elevator may also be used as a straight elevator (Fig. 4.52 a). The straight Chompret elevator may only be used this way
Fig. 4.53. Sharp-tipped angled elevators suitable for removal of root tips
when the width of the straight elevator blade prevents its correct placement for the luxation of the tooth or root.
Curved Chompret Elevator (Fig. 4.52 b) and Doubleangled Elevators with Narrow Blades and SharpTipped Ends (Fig. 4.53). These instruments are used by the dentist as the need dictates.
Chapter 4 Equipment, Instruments, and Materials |
63 |
Fig. 4.54 a, b. a Special instrument for removing roots below the margin of alveolar bone. b Bur for widening the root canal
Fig. 4.55. Periapical curettes with ends of different sizes
Fig. 4.56 a,b. Desmotomes. a Straight. b Curved
4.22 |
4.24 |
Special Instrument for Removal of Roots |
Desmotomes |
The instrument in Fig. 4.54 is used to remove broken roots found below the alveolar crest. The spiral end of the instrument is placed inside the extraction socket, and, after screwing the instrument into the root canal of the broken root, traction is used to remove the root from the socket (see Chap. 5).
These instruments are used to sever the soft tissue attachment, and are either straight or curved (Fig. 4.56 a, b). The straight desmotome is used for the anterior teeth of the upper jaw and the curved desmotome for the rest of the teeth of the upper jaw as well as all of the teeth of the lower jaw.
4.23
Periapical Curettes
These are angled double-ended, spoon-shaped instruments (Fig. 4.55). The most commonly such used instrument is the periapical curette, whose shape facilitates its entry into bone defects and extraction sockets.
The main use of this instrument is the removal of granulation tissue, small cysts, bone chips, foreign bodies, etc.